
Specifics of Female Acne

The Essential Info
Hormones/Premenstrual: Hormones fluctuate more in women than in men due to the menstrual cycle. Women tend to see a flare in acne 7-10 days before menstruation begins.
Adult acne: Compared to only about 1/4 of adult men, more than 1/2 of adult women experience breakouts.
Pregnancy: During pregnancy, women normally see less acne, but acne may flare in the 3rd trimester.
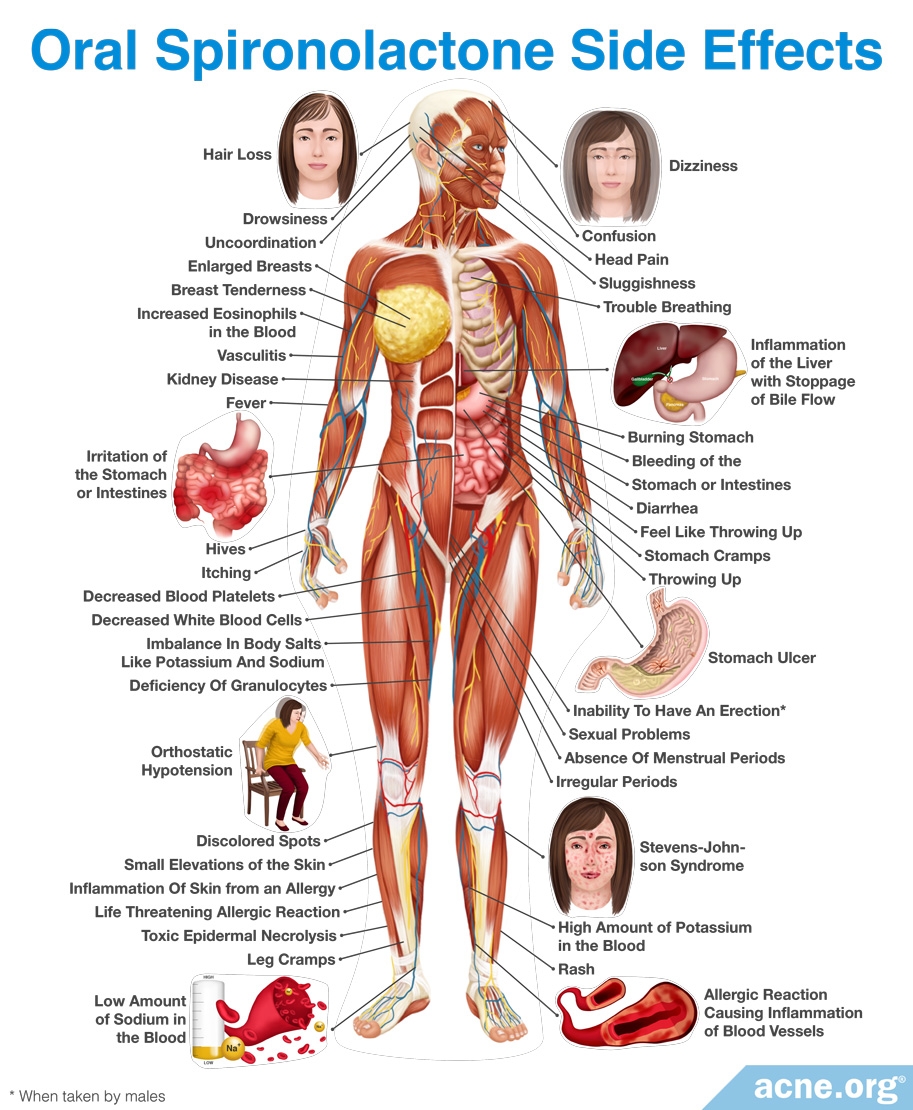
Hormonal treatment: Hormonal treatment, including oral contraceptives (birth control pills), and anti-androgen medications like spironolactone are an option for females only. They are particularly helpful if you notice menstrual irregularities and/or excessive hair growth, which can be symptoms of poly-cystic ovary syndrome.
EXTREME CAUTION: NEVER TAKE THE ORAL MEDICATION ISOTRETINOIN (ACCUTANE) IF YOU ARE PREGNANT OR PLANNING TO BECOME PREGNANT. IT CAUSES SEVERE BIRTH DEFECTS.

The Science
- 5 Facts about Female Acne
- Premenstrual
- Menopause
- Pregnancy
- Treatment Options
- Hormonal Treatment: Birth Control (Oral Contraceptives)
- Spironolactone
- Cyproterone Acetate (Diane-35)
5 Facts about Female Acne:
- As a general rule, women’s hormones tend to fluctuate more than men’s, which helps explain why acne in women tends to be less constant and more erratic than acne in men.
- More than half of all adult women experience at least occasional breakouts.
- 60-70% of women who battle acne experience premenstrual flare-ups.
- Acne can occur throughout a woman’s adult life: in early adulthood, in the late twenties and thirties, during pregnancy, and during menopause.
- Female adult acne can be frustrating, but can be effectively treated.
Premenstrual

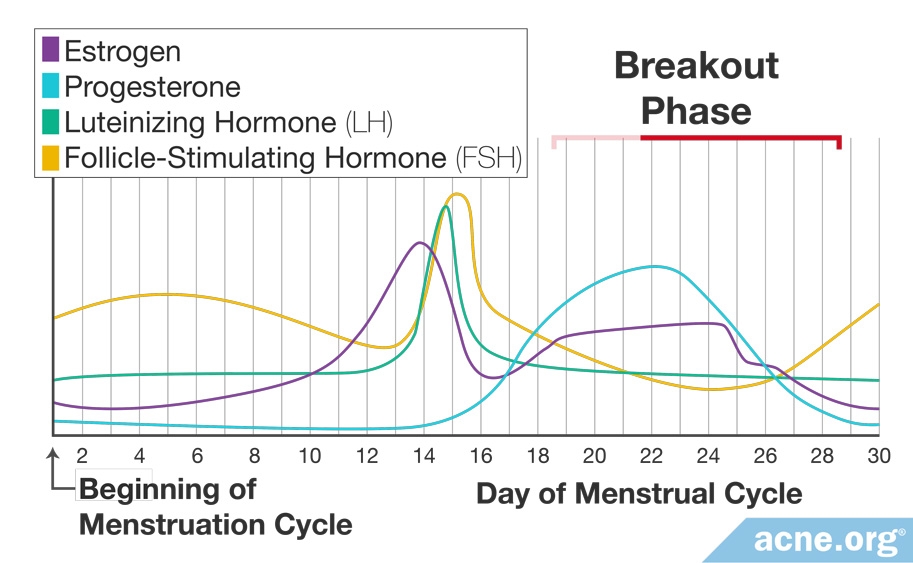
A study published in the Archives of Dermatology in 2004 showed 63% of acne-prone women experiencing premenstrual flares, with a 25% increase in total lesions.1 This probably comes as no surprise to the millions of women out there who experience a monthly flareup of their acne symptoms. Normally there is an increase in acne about 7-10 days before the onset of menstruation and often subsides when menstruation begins. Multiple studies have confirmed and acknowledged the occurrence of premenstrual acne. No one is sure exactly why this occurs, but it’s safe to say that it has something to do with the intricate hormonal changes involved in the menstrual cycle.
The key hormones involved in the menstrual cycle are estrogen and progesterone (female hormones that are present in both males and females). Some studies suggest that estrogen may reduce sebum production and act as an anti-inflammatory agent. On the other hand, a rise in progesterone prior to the onset of menstruation is thought to be responsible for the premenstrual flare-ups.
When it comes to premenstrual acne, prevention is key. Because hormonally-induced acne can be hard to treat, there may be no way to completely combat it, but The Regimen does a fantastic job at turning a monthly scourge into a blip, or even eliminating it entirely. Birth control pills and androgen receptor blockers may also help with regulating hormones.
Menopause
Any time people experience a change in hormones, they usually experience breakouts. The general trend is that following adolescence, the occurrence of acne steadily decreases over the years. This decrease continues through menopause. However, due to fluctuation in hormone levels around and during menopause, some women may notice a slight flare in their existing acne in this period. This normally subsides once menopause has run its course.
On the other hand, if you experience new onset acne or a significant worsening in existing acne after menopause, it may indicate an underlying medical condition such as a tumor or a reaction to some medication you are taking. If this is the case, it is important to see your doctor as soon as possible to rule out the other conditions that may be causing the acne symptoms.
Pregnancy

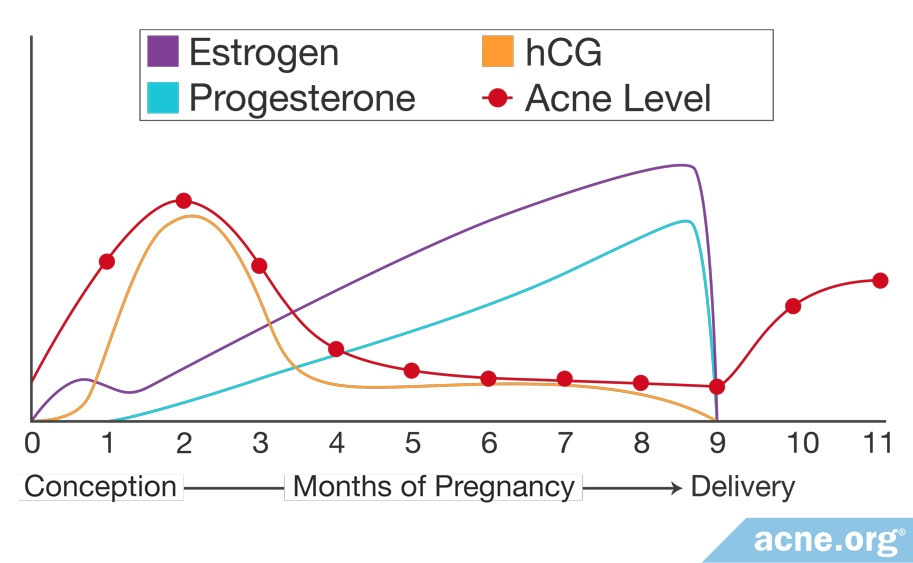
Typically, women who suffer from acne see an improvement in their condition in the early months of pregnancy, possibly owing to the increase in estrogen levels, which is thought to have an anti-inflammatory effect. During the later stages of pregnancy, particularly in the third trimester, there is generally worsening of acne. This is thought to occur because of the increase in androgen (male sex hormones present in both males and females) levels during this period of the pregnancy. High androgen levels are associated with acne. But don’t worry too much because this trend is not the same for all women and can even vary between pregnancies in the same woman. After childbirth, the changes in the acne severity that occurred during the pregnancy usually revert to the baseline (acne severity in the pre-pregnancy state).1-2
Treatment options: First, talk to your doctor. The vast majority of acne treatments, both prescription and over-the-counter, have not been studied in pregnant or lactating mothers. Your doctor may have options for you that he/she considers safe for use during your pregnancy.
EXTREME CAUTION!: One option that is absolutely unsafe is Accutane (isotretinoin). The active ingredient in Accutane, isotretinoin, is highly teratogenic (causes birth defects).3 It is absolutely vital that women who are pregnant or plan to become pregnant avoid isotretinoin.
Your baby: Yes, even babies can have acne. It is referred to as neonatal acne and it normally subsides on its own.4 If your son or daughter shows signs of acne as an infant, they may also suffer from acne as an adolescent. Be sure to have an open and honest talk with them if they start breaking out as a teenager and explain their options.
Hormonal Treatment Options
For many women, the right topical medications can keep acne at bay. Men and women do not differ significantly in terms of effective acne treatments, and appropriate application of topical treatment is often the best option.
Hormonal treatments are also an option.1-3 Doctors sometimes prescribe oral contraceptives (birth control pills), or androgen receptor blocker (most notably spironolactone and cyproterone acetate). Both oral contraceptives and androgen receptor blockers work internally to mediate the effects of male hormones, which are integral in the development of acne. Both options come with numerous side effects and should be carefully researched and then discussed with a trusted physician before coming to an educated decision on whether or not to embark on hormonal therapy.
As a last resort, for women with very severe, widespread, and deeply scarring acne, Accutane (isotretinoin) is also an option. However, because Accutane causes severe birth defects in the fetuses of pregnant women, and because of Accutane’s other serious side effects. Accutane treatment should be entered into carefully. Before taking Accutane, make sure to have a thorough discussion with your family and your doctor and become as educated as possible on the drug.
Hormonal Treatment: Birth Control (Oral Contraceptives)

How do oral contraceptives (OCs) help with acne? As a general rule, OCs reduce androgens (male sex hormones present in both males and females) which are partly responsible for acne formation. Women with acne tend to have higher levels of androgens.1-5 More specifically:
- OCs reduce the level of free testosterone (a form of androgen) in a woman’s body by signaling the ovaries and adrenal gland to produce less.2
- OCs increase the level of SHBG (sex hormone-binding globulins), which are proteins that inhibit the conversion of free testosterone into dihydrotestosterone (DHT, another type of androgen). In short, there is less DHT in the body.1,3
- The progestin component of OCs lower androgen levels.2
Which work best? The FDA has approved only a select handful of birth control pills for patients with acne who also desire contraception. They include Ortho Tri-Cyclen, Estrostep, and Yaz. However, all birth control pills tend to produce 30%-60% reduction in acne lesions, and research remains inconclusive on which works best.3,6-11
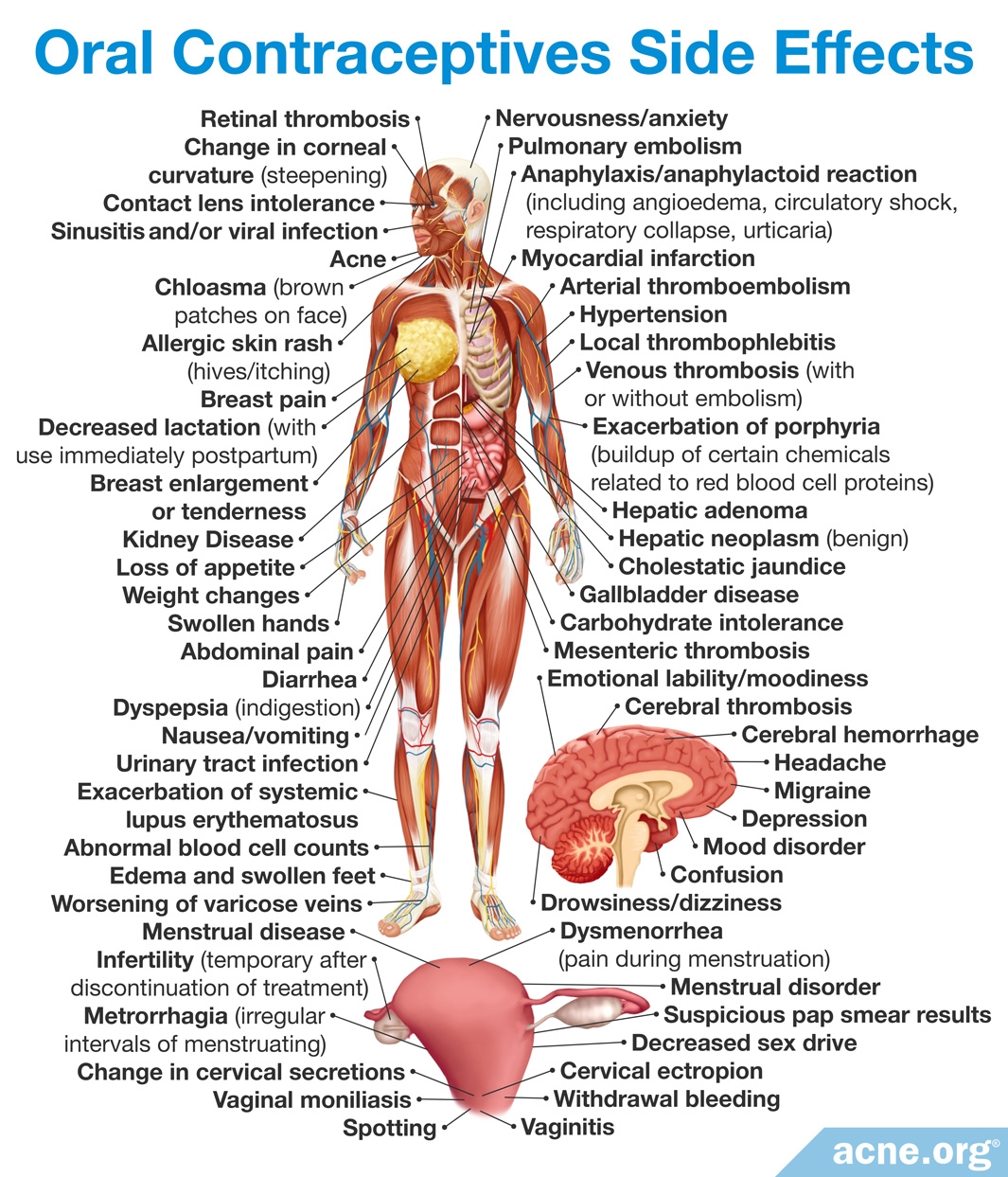
What are the side effects? Side effects are common. Some of the more common ones include nausea, headache, breast tenderness, breakthrough bleeding (bleeding that occurs in between the normal menstrual periods), bloating, fatigue, irritability, mood changes, dizziness, weight gain, loss of libido, high blood pressure, and vaginal infections. Less common, serious side effects include blood clots, heart problems (exacerbated by smoking), and possibly increased cancer risk.10,12 Talk to your doctor for more information.
Do antibiotics cause birth control pills to fail? While this is a largely held belief, and women have indeed become pregnant with the combination of birth control pills and antibiotics (tetracyclines), but pregnancy rates were no higher than that seen from birth control pill failure alone. According to a 2010 overview article published in the International Journal of Women’s Health, ” Currently, there are no pharmacokinetic data or randomized controlled clinical trials supporting that oral antibiotics decrease the efficacy of oral contraceptives, with the notable exception of anti-tuberculosis drugs like rifampin.”3
Spironolactone

What it is: Women who experience acne tend to have higher levels of androgens (male sex hormones present in both males and females). Spironolactone is an androgen receptor blocker. In other words, it prevents the cells of the body from interacting with androgens. Less androgens typically means less acne.1-3 Spironolactone is taken in pill form and can be used with other topical acne treatments, as well as in conjunction with birth control pills. It is especially effective when excessive hair growth (hirsutism) is present. Spironolactone is also used to treat this condition.4
Study results: Spironolactone has shown mixed results in several studies, both on its own and coupled with oral contraceptives.
Two recent studies found spironolactone effective in reducing acne.5,6
Expand to read details of studies

In a study published in 2009 in the Journal of the American Academy of Dermatology in 2008, 85% of women achieved very good results with a combination of spironolactone and an oral contraceptive with drospirenone.5

Another study published in the Journal of the European Academy of Dermatology and Venereology showed “clinically significant improvement” in 85.71% of subjects taking spironolactone alone.6
However, other studies have shown no significant decrease in acne symptoms when using spironolactone alone.

Due to the small number of studies in this area, and their conflicting results, the authors of a meta-analysis in 2009, published in The Cochrane Library, conclude, “there [is] no evidence for the effectiveness of [spironolactone] for the treatment of acne vulgaris.”3
Side effects: Side effects are common. Studies show upwards of 50% of women experiencing menstrual irregularities. Spironolactone may create breast tenderness, headache, or fatigue, and can also have a diuretic effect. In pregnant women, feminization of the male fetus is also possible.6

However, an 8-year study published in the Journal of Cutaneous Medicine and Surgery concluded, “…there were no cases of serious illness attributable to spironolactone use.”7
Note: Asian women sometimes respond differently to hormonal treatment. However, a study of 116 Japanese women completed in 2006 showed that “…spironolactone is effective and safe for the treatment of acne in Asian females.”8
Men: Spironolactone is usually reserved for use in females because gynecomastia (male breast growth) can occur in males who take the drug.
Cyproterone Acetate (Diane-35)
What it is: Acne-prone women tend to have higher levels of androgens (male sex hormones). Cyproterone acetate is an anti-androgen, which helps suppress the male sex hormones testosterone and dihydrotestosterone (DHT). Less androgens typically means less acne.1 Cyproterone acetate is administered in pill form and also sometimes as a topical lotion. In both forms it has been shown to reduce sebum (skin oil) production. It can normally be used alongside other topical acne treatments. It is also used to treat polycystic ovary syndrome, excessive hair growth (hirsuitism), alopecia, and other diseases where androgen action is involved. Cyproterone acetate is a main ingredient in Diane-35 (cyproterone acetate plus ethinyl estradiol), a popular oral contraceptive in Europe and Canada.
Study results: The two studies performed thus far have shown 75%-90% of women experiencing an improvement in acne symptoms when taking cyproterone acetate alone.2-3 Another study found that women using Diane-35 saw a 58.8% decrease in total acne lesion count.4
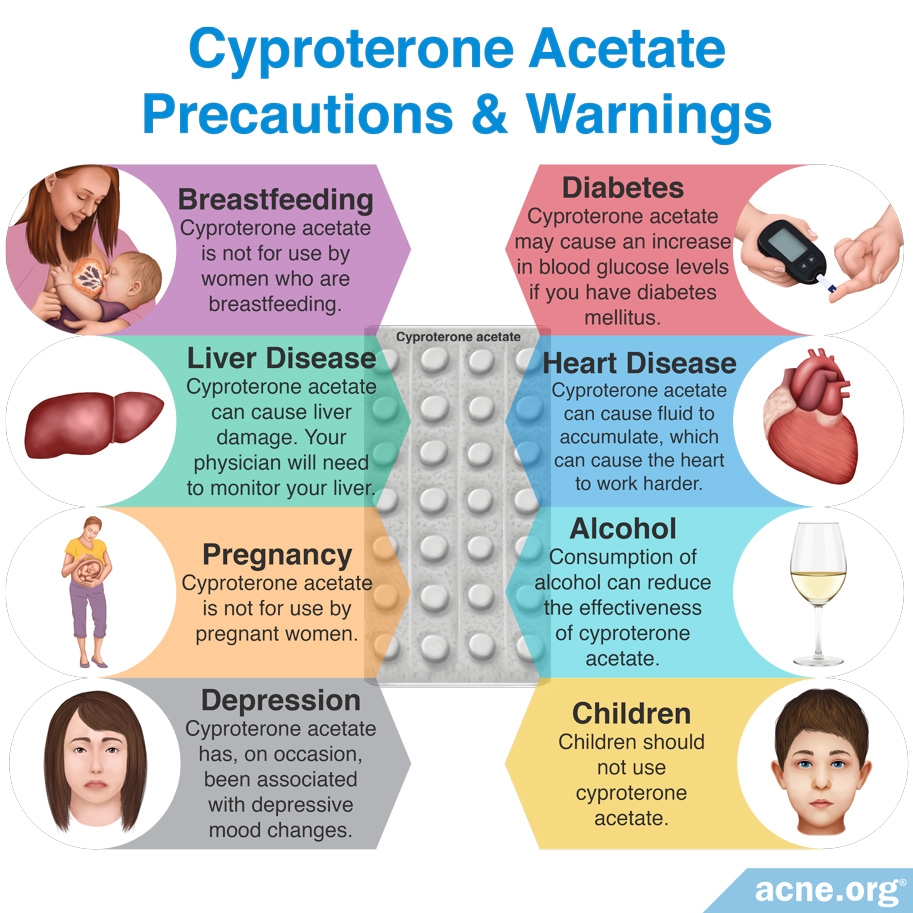
Side effects: The most notable side effect is liver toxicity. In combination with oral contraceptives, there is an increased risk of blood clots. Osteoporosis is also a potential side effect with long-term use.
Note: Asian women sometimes respond differently to hormonal treatment. If you are of Asian descent, be sure to ask your doctor if he/she is aware of your particular circumstance before embarking on treatment.
Men: Cyproterone acetate is usually reserved for use in females because gynecomastia (male breast growth) and galactorrhea (milk production) may occur in males who take the drug.
References
Premenstrual:
- Lucky, A. W. Quantitative documentation of a premenstrual flare of facial acne in adult women. Arch. Dermatol. 40, 423-424 (2004). https://www.ncbi.nlm.nih.gov/pubmed/15096370
Pregnancy:
- Fulton, J. E. Acne Rx (James E. Fulton Jr., M.D., PhD, 2001).
- Bozzo, P., Chua-Gocheco, A. & Einarson, A. Safety of skin care products during pregnancy. Can. Fam. Physician 57, 665-667 (2011). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3114665/
- Honein, M. A., Paulozzi, L. J. & Erickson, J. D. Continued occurrence of Accutane-exposed pregnancies. Teratology 64, 142-147 (2001). https://www.ncbi.nlm.nih.gov/pubmed/11514944
- Hello, M. et al. Infantile acne: A retrospective study of 16 cases. Pediatr. Dermatol. 25, 434-438 (2008). https://www.researchgate.net/publication/227773934_Infantile_Acne_A_Retrospective_Study_of_16_Cases
Further Reading
- Roche Accutane (isotretinoin capsules). Roche Laboratories, Inc. Oct. 2007. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3970835/
Treatment Options:
- Shaw, J. C. & White, L. E. Persistent Acne in Adult Women. Arch. Dermatol. 137, 1252-1253 (2001). https://www.ncbi.nlm.nih.gov/pubmed/11559234
- Rivera, R & Guerra, A. [Management of acne in women over 25 years of age]. Actas Dermosifiliograf. 100, 33-37 (2009). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5798558/
- Salvaggio, H. L. & Zaenglein, A. L. Examining the use of oral contraceptives in the management of acne. Int. J. Womens Health. 2, 69-76 (2010). https://www.ncbi.nlm.nih.gov/pubmed/21072299
Further Reading
- Fulton, J. E. Acne Rx (James E. Fulton Jr., M.D., PhD, 2001). 107-115.
- Preston, L. Breaking Out: A Woman’s Guide to Coping with Acne at Any Age (Fireside, 2004). https://www.researchgate.net/publication/26183445_Breaking_Out_A_Woman’s_Guide_to_Coping_with_Acne_at_Any_Age
Hormonal Treatment: Birth Control (Oral Contraceptives):
- Lemay, A. & Poulin, Y. Oral contraceptives as anti-androgenic treatment of acne. J. Obset. Gynecol. Can. 24, 559-567 (2002). https://www.ncbi.nlm.nih.gov/pubmed/12196847
- Shaws, J. C. Acne: effect of hormones on pathogenesis and management. Am. J. Clin. Dermatol. 3, 571-578 (2002). https://www.ncbi.nlm.nih.gov/pubmed/12358558
- Salvaggio, H. L. & Zaenglein, A. L. Examining the use of oral contraceptives in the management of acne. Int. J. Womens Health. 2, 69-76 (2010). https://www.ncbi.nlm.nih.gov/pubmed/21072299
- Cameron, S. Contraception and gynaecological care. Best Pract. Res. Clini. Obstet. Gynaecol. 23, 211-220 (2009). https://www.ncbi.nlm.nih.gov/pubmed/19147411
- Harper, J. Should dermatologists prescribe hormonal contraceptives for acne? Dermatol. Ther. 22, 452-457 (2009). https://www.ncbi.nlm.nih.gov/pubmed/19845722
- Poulin Y. Practical approach to the hormonal treatment of acne. J. Cutan. Med. Surg. 8 Suppl 4,16-21 (2004). https://www.ncbi.nlm.nih.gov/pubmed/15778820
- Tan, J. Hormonal treatment of acne: review of current best evidence. J. Cutan. Med. Surg. 8 Suppl 4, 11-15 (2004). https://europepmc.org/abstract/med/15778821
- Tan, J. K. New developments in hormonal therapy for acne. Skin Therapy Lett. 12, 1-3 (2007). https://www.ncbi.nlm.nih.gov/pubmed/17940710
- Van Vloten, W. A. & Sigurdsson, V. Selecting an oral contraceptive agent for the treatment of acne in women. Am. J. Clin. Dermatol. 5, 435-441 (2004). https://www.ncbi.nlm.nih.gov/pubmed/15663340
- Katsambas, A. D. & Dessinioti, C. Hormonal therapy for acne: Why not as first line therapy? Facts and controversies. Clin. Dermatol. 28, 17-23 (2010). https://www.ncbi.nlm.nih.gov/pubmed/20082945
- Maloney, J. M. et al. Treatment of acne using a 3-milligram drospirenone/20-microgram ethinyl estradiol oral contraceptive administered in a 24/4 regimen. Obstet. Gynecol. 112(4): 773-781 (2008). https://www.ncbi.nlm.nih.gov/pubmed/18827119
- Estrogen and Progestin (oral contraceptives). Medline Plus. American Society of Health-Systems Pharmacists, Inc. 2011. https://medlineplus.gov/druginfo/meds/a601050.html
Further Reading
- O’Connell, K. & Westhoff, C. Pharmacology of hormonal contraceptives and acne. Cutis. 81(1 Suppl): 8-12 (2008). https://www.ncbi.nlm.nih.gov/pubmed/18338652
- Rich, P. Hormonal contraceptives for acne management. Cutis. 81(1 Suppl): 13-8 (2008). https://www.ncbi.nlm.nih.gov/pubmed/18338653
Spironolactone:
- Bagatin, E. dos Santos Guadanhim, L. R., Yarak, S., Kamamoto, C. S. & de Almeida, F. A. Dermabrasion for acne scars during treatment with oral isotretinoin. Dermatol. Surg. 36, 483-489 (2010). https://www.ncbi.nlm.nih.gov/pubmed/20180836
- Bhalla, M. & Thami, G. Microdermabrasion: Reappraisal and brief review of literature. Dermatol. Surg. 32, 809-814 (2006). https://www.ncbi.nlm.nih.gov/pubmed/16792646
- Carniol, P., Meshkov, L. & Grunebaum, L. Laser treatment of facial scars. Curr. Opin. Otolaryngol. Head Neck Surg. 19, 283-288 (2011). https://www.ncbi.nlm.nih.gov/pubmed/21659876
- Chandrashekar, B. & Nandini, A. Acne scar subcision. J. Cutan. Aesthet. Surg. 3, 125-126 (2010). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2956956/
- Cho, S, Lee, H. J., Choi, M. J., Lee, K. Y. & Oh, S. H. Efficacy of the fractional photothermolysis system with dynamic operating mode on acne scars and enlarged facial pores. Dermatol. Surg. 35, 108-114 (2009). https://www.ncbi.nlm.nih.gov/pubmed/19076205
- Costa, I., Salaro, C., & Costa, M. Polymethymethacrylate facial implant: A successful personal experience in Brazil for more than 9 years. Dermatol. Surg. 35, 1221-1227 (2009). https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1524-4725.2009.01216.x
- Doddaballapur, S. Microneedling with dermaroller. J. Cutan. Aesthet. Surg. 2, 110-111 (2009). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2918341/
- Emsen, I. An update on sandpaper in dermabrasion with a different and extended patient series. Aesthet. Plast. Surg. 2008. https://www.ncbi.nlm.nih.gov/pubmed/18498010
Cyproterone Acetate:
- Katsambas, A. D. & Dessinioti, C. Hormonal therapy for acne: Why not as first line therapy? Facts and controversies. Clin. Dermatol. 28, 17-23 (2010). https://www.ncbi.nlm.nih.gov/pubmed/20082945
- Van Wayjen, R. G. & Van Den Ende, A. Experience in the long-term treatment of patients with hirsutism and/or acne with cyproterone acetate-containing preparations: Efficacy, metabolic and endocrine effects. Exp. Clin. Endocrinol. Diabetes. 103, 241-251 (1995). https://www.ncbi.nlm.nih.gov/pubmed/7584530
- Gollnick, H., Albring, M. & Brill, K. The effectiveness of oral cyproterone acetate in combination with ethinyl estradiol in acne tarda of the facial type. Ann. Endocrinol (Paris). 60, 157-166 (1999). https://www.ncbi.nlm.nih.gov/pubmed/10520404
- Ebede, T. L., Arch, E. L. & Berson, D. Hormonal Treatment of Acne in Women. J. Clin. Aesthet. Dermatol. 2, 16-22 (2009). https://www.ncbi.nlm.nih.gov/pubmed/20725580

{kind=link}
{kind=link}