Acne.org Products
Acne.org Productsanother thing worth mentioning is that I have began to exercise and lift weights fairly heavily the past few weeks, and I am wondering if perhaps this is affecting something. For example, I was just finished lifting weights, and that seems to have at least helped the problem somewhat with what I think was the prolactin.
Also, I wouldnt call what Im dealing with depression per say. I dont have a low mood as much as no mood, and I dont feel lethargic either.
On 4/25/2019 at 9:59 PM, cnb30 said:I dont think Ive had too many vision problems, although the tumor would make sense as I remember people mentioning it as a possible Finasteride side effect. Also, it feels as though someone is slowly secreting some sort of cold mist through my dopamine passageways as well (if thats what prolactin feels like). You arent the first person to have mentioned increased prolactin either, but that would make sense.
Is there anything I can do about it? Im kinda back at a point where I feel as though Im at the end of a string, and I dont want to live anymore if it means being in the state Im currently in.
I also took Abilify for a time, and I know that increases prolactin levels too, right?
Also, I should add that I dont really have the money or time to get these tests done, and dont know how the hell to convince my parents.
Prolactin is very interconnected with dopamine. So, assuming you have elevated prolactin levels, increasing dopamine would be a way to effectively treating elevated prolactin. This is an actual way of treating/getting rid of prolactinomas actually: They usually give you a drug named Cabergolin which is a dopamine agonist (meaning it mimics the effects of dopamine).
On 4/26/2019 at 12:04 AM, cnb30 said:another thing worth mentioning is that I have began to exercise and lift weights fairly heavily the past few weeks, and I am wondering if perhaps this is affecting something. For example, I was just finished lifting weights, and that seems to have at least helped the problem somewhat with what I think was the prolactin.
Also, I wouldnt call what Im dealing with depression per say. I dont have a low mood as much as no mood, and I dont feel lethargic either.
Exercising is known to increase dopamine, so it makes sense that you feel better after exercising. Although, exercising too much can also elevate prolactin since prolactin can be categorized as a stress response hormone (it increases in concentration due to things such as mental and physical stress).
Also, I personally have elevated prolactin levels, and I know there are many theories going around on this forum and others, but I personally believe that for accutane, the sexual side effects are due mainly because of dopamine/serotonin disruption. We know for a fact that Accutane has the ability to negatively influence the dopamine circuity of our brains (I'll link the study if you'd like), and it also effects serotonin aswell. I feel like this could also partially explain why people believe it's the Androgren receptor being down regulated that's causing our symptoms because serotonin is known to be a potent AR inhibitor.
Also i know people have mentioned the D2 receptor and what not as being something of importance, but I don't believe it's getting the amount of attention that it should be getting.
If you'd like, pm me and I'll discuss my theory more.
Edit: Here are some links to studies discussing Accutane and dopamine
Accutane's effect on D2 receptor (although it doesn't entirely focus on it, just ctrl-f "D2): https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2637283/
On 4/20/2019 at 10:00 PM, Dubya_B said:On a related note, something surprising I stumbled upon last Summer shows an effect of ATRA on neurosteroidogenesis in glial cells contradictory to what one would expect after studies have shown decreased hippocampal neurogenesis after ATRA treatment:
sorry for the long pause. Maybe the paradoxes come into effect looking at a higher sustained dose such as Accutane.
All-Trans-Retinoic AcidAugments the Histopathological Outcome of Neuroinflammation and Neurodegeneration inLupus-Prone MRL/lpr Mice. Show all authors.
What's one of the mechanisms?
More than half your body is not human - BBC News - BBC.com
https://www.bbc.com/news/health-43674270
The field is even asking questions of what it means to be "human" and is leading to new innovative treatments as a result.
Genetically we're even more outgunned.
The human genome - the full set of genetic instructions for a human being - is made up of 20,000 instructions called genes.
But add all the genes in our microbiome together and the figure comes out between two and 20 million microbial genes.
Prof Sarkis Mazmanian, a microbiologist from Caltech, argues: "We don't have just one genome, the genes of our microbiome present essentially a second genome which augment the activity of our own.
"What makes us human is, in my opinion, the combination of our own DNA, plus the DNA of our gut microbes."
You're right @guitarman01. I was thinking along these lines but kept erroneously referring to an effect that explains a paradoxical response to excessive doses as inverse-agonism.
Seriously, it was right under my nose and didn't realize it. This biphasic/hormetic effect has been observed of alloregnanolone and testosterone and a persistently decreased set-point for this effect was discussed as an explanation for the adverse reaction some PFS patients have to increasing testosterone:
https://en.wikipedia.org/wiki/Allopregnanolone
QuoteIncreased levels of allopregnanolone can produce paradoxical effects, including negative mood, anxiety, irritability, and aggression.[17][18][19] This appears to be because allopregnanolone possesses biphasic, U-shaped actions at the GABAA receptor moderate level increases (in the range of 1.52 nM/L total allopregnanolone, which are approximately equivalent to luteal phase levels) inhibit the activity of the receptor, while lower and higher concentration increases stimulate it.
[removed]
Most importantly, Retinoic Acid, (and presumably Accutane), has been shown to exert this type of effect on GnRH receptors:
Good news, the prolactin issue has appeared to mostly go away! Also, Ive been in a state the pastweekwhere I feel like Ive recovered some past sensations too!
Nice!
Did the high prolactin levels go down on their own, or did you take something to lower them?
I took a dopamine agonist, bromocriptine, for around 4-5 years after having borderline high prolactin on a few blood tests, and it seemed to help a little.
It was a band aid treatment, and it didn't seem to do anything beneficial the most recent couple times I tried taking it, but anything is better than nothing and it was good while it lasted.
.
On 5/5/2019 at 10:30 AM, TrueJustice said:Isnt the origin of prolactin issues a problem with pituitary gland??
HPA Axis dysfunction mentioned many times on forum,anyone tried to work with a specialist to fix this issue?
Or happy to self diagnose and experiment for years on end....
Which specialist are we seeing?
I Agree,
People might want to see their GP for a prolactin blood test if they think this is an issue for them. That's how I know my prolactin is normal.
I think youve mentioned youve got a good GP.
Yes Ill go to mine to getblood tests donebut in terms of rebuilding my health, thats where it ends.
Happy to seek a specialist outside of the mainstream who knows how to interpret those blood tests and actually help me make improvements. Someone who knows what to take and when which means I can at least eliminate self diagnosing
On 5/2/2019 at 10:03 PM, Dubya_B said:You're right @guitarman01. I was thinking along these lines but kept erroneously referring to an effect that explains a paradoxical response to excessive doses as inverse-agonism.
Seriously, it was right under my nose and didn't realize it. This biphasic/hormetic effect has been observed of alloregnanolone and testosterone and a persistently decreased set-point for this effect was discussed as an explanation for the adverse reaction some PFS patients have to increasing testosterone:
So has anyone you know of actually been diagnosed with any kind of nerve damage or blood vessel disorder?
Have metabolic markers been looked at extensively in PFS?
Speaking of Paradoxes, how to distinguish if looking for something life changing?
Because there might have been a problem even before we took accutane, or other said drugs.
It is important to differentiate thistinglingfrom the pain sometimes produced by pressure on an injurednerve. The pain is a sign of irritation of thenerve;tinglingis a sign of regeneration; or more precisely,tinglingindicates the presence of young axons, in the process of growing.
on inflammation and pain. without pain there can be no healing. the problem is when it becomes chronic, without the healing process.
Inflammationis part of the body's immune response. Infections, wounds, and any damage to tissue would not be able to heal without aninflammatoryresponse. Chronicinflammationcan eventually cause several diseases and conditions, including some cancers and rheumatoid arthritis.Nov 24, 2017
I still think this could be the next direction.
Scientists succeed in deciphering microbiome contributions to drug metabolism
It is a well-known fact thata broad range of drugscan affect gut microbiota composition. Furthermore, the gut microbiome may affect drug efficacy and toxicity
let me quickly elaborate on my last post.
inflammation as a sign of healing? nerve tingling as a sign of healing?
or just a worsening of symptoms? How do you tell which one is which.
(oh, BTW, dry skin could very much so have neurological involvement.)
Your body needs to know exactly where the problems are to generate this inflammation and appropriate response.
immune homeostasis.
An inflammation that dissipates over time.
Let me give an example
Bifidobacterium's capacity to stimulate immunity is species specific, but its influence on the orientation of the immune system is strain specific.
The anti inflammatory effect of these bacteria is believed to be one of the strategies required for their successful colonization of the hosts intestine, overcoming the natural defense barrier, including inflammation. therefore the increase of the bacteria, including bifidobacteria, which can enhancethe intestinal inflammation in aged people, can be considered a beneficial response of the host to such an age related change in their intestinal microecology. this may contribute to the homeostasis of local immunity by preventing local inflammation from being over suppressed.
im still focused on this genus of bacteria for a few reasons.
Heres one.
Bifidobacterium longumsubsp.infantis35624 (B. infantis) was originally isolated from resected human healthy gastrointestinal tissue and human clinical studies have demonstrated its efficacy in Irritable Bowel Syndrome patients[15],[16]. In addition, murine studies have demonstrated that this microbe protects against inflammatory disorders across a range of inflammatory conditions including colitis, pathogen infection, arthritis and respiratory inflammation[17][20]. Previously,in vitrostudies with human dendritic cells suggested that promotion of retinoic acid metabolism byB. infantiswas a key regulatory feature of this bacterium[21]
So again friend or foe?
This is an antibiotic resistant strain btw. many in the b.longum family seem to be
promote metabolism. you can look back to my previous study. That could be good or bad.
But whats in the definition of metabolism?
To break down.
Heres another one.
Did you guys know this?
On 5/7/2019 at 8:40 PM, guitarman01 said:So has anyone you know of actually been diagnosed with any kind of nerve damage or blood vessel disorder?
Have metabolic markers been looked at extensively in PFS?
Speaking of Paradoxes, how to distinguish if looking for something life changing?
Because there might have been a problem even before we took accutane, or other said drugs.
Off the top of my head, I've never heard of a PAS patient mention being DX'ed with either nerve damage or a blood vessel disorder.
Metabolic markers have been thoroughly investigated in PFS patients, considering the number of them who have shared blood work results. Nothing consistently out of the ordinary has emerged in that respect.
Not quite certain what you mean by the next to last statement. The only way to tell what was happening would be to wait and see if you improved or worsened. ...Unless you had some means to test for signs of neuropathy.
On the last point; what problem? As a general statement it can be said that we were all young people in good health before taking Accutane. ...Unless you want to consider acne a pathological condition. What harm does it bring to the host with the possible exception of psychological distress that is often blown out of proportion compared to the severity of acne by proponents of Accutane?
I tried to find some evidence that Accutane might induce pathological changes in the microbiome and all I could come up with were a few studies showing a significant reduction of P. acnes, and a study someone sent me showing an effect on the gut microbiome that wasn't only insignificant, but negligible:
E. Becker et al., Effects of oral antibiotics and isotretinoin on the murine gut microbiota, International Journal of Antimicrobial Agents, vol. 50, no. 3, pp. 342351, Sep. 2017.
Quote
In faecal samples collected prior to the start of treatment, there were no notable differences between the treatment and vehicle- control groups for either of the antibiotics (metronidazole, doxycycline and water; multi-variate analysis of variance on phylum-level tax- onomic composition, F = 2.01, P = 0.0673) or isotretinoin (isotretinoin and rapeseed oil; F = 0.407, P = 0.802) treatment regimen. Follow- ing 2 weeks of treatment, microbiota composition at phylum level differed significantly between the antibiotic groups (F = 3.87, P = 0.002); this difference persisted after the recovery period (F = 2.62, P = 0.016). In contrast, isotretinoin treatment did not induce significant changes from pretreatment composition either immediately after treatment (F = 1.01, P = 0.419) or after the recovery period (F = 1.55, P = 0.25). Notably, mice treated with water or antibiotics showed generally elevated Firmicutes levels after the recovery period compared with mice treated with isotretinoin or rapeseed oil vehicle.
.
Dubya_b and guitarman01 -
I just want to point something out regarding all this talk of bacteria and accutane.
Folliculitis is so common after accutane even in people that have never had folliculitis before.
Antibiotics suppress folliculitis, not permanently but while on it.
So its either bacteria or inflammation, now pregnisone or cortef or cortisol etc also suppress it.
Accutane will remove folliculitis but ive read it comes back.
I recently saw a dermatologist about it and they mentioned accutane or antibiotics again.
I always thought it was a low cortisol/inflammation thing but now I'm wondering is it a gut bacteria thing?
Like 12 months after accutane maybe there is too much of a certain type of bacteria?
Any ideas?
Well, H.Pylori has been found easy enough in post Accutane victims
Dont know if you can test yourself, my kinesiologist was able todetect it easy enough though.
All part of breaking down biofilms - viruses, fungus and bad bacteria and rebuilding the gut.
As long as youre working with a good specialist youll be right, if youre not um.......
3 hours ago, TrueJustice said:Well, H.Pylori has been found easy enough in post Accutane victims
Dont know if you can test yourself, my kinesiologist was able todetect it easy enough though.
All part of breaking down biofilms - viruses, fungus and bad bacteria and rebuilding the gut.
As long as youre working with a good specialist youll be right, if youre not um.......
Actually I can report some improvements on antibiotics, so maybe it is bad bacteria causing HPA axis disfunction.
What I don't get is why it started after treatment, ideas?
Maybe this bad bacteria is reduced by fasting?
Youd be best to look up the causes of HPA dysfunction- there are probably many ways one can get it and different ways of combating it. Im making improvements for sure with my weekly treatment.
Not sure about you but in terms of dryness Ive made no progress whatsoever, I can be honest about that -skin on face is clear but super dry. I really think Imresigned to the fact that my sebaceous glandsare forever changed from Accutane, theres just none of that natural oil in my skin anymore unfortunately
Ive not spent any time talking to kinesiologist about it as Id rather they continue to work on things they can fix and identify in me.
Dry skin, eye floaters I doubt after 20 years theyll ever improve, Ill just try and concentrate on what is working- I dont know of any better approach right now.
18 hours ago, Dubya_B said:I tried to find some evidence that Accutane might induce pathological changes in the microbiome and all I could come up with were a few studies showing a significant reduction of P. acnes, and a study someone sent me showing an effect on the gut microbiome that wasn't only insignificant, but negligible:
I'll see your study and I'll raise you a few more. I really dont need further studies on any of this though when looking at what might be possible.
The effects of systemic isotretinoin and antibiotic therapy on the microbial floras in patients with acne vulgaris.
https://www.ncbi.nlm.nih.gov/pubmed/22239608
CONCLUSIONS:
Systemic isotretinoin and antibiotic treatments in acne patients precisely caused variations in the microbial floras of several sites of the body, while isotretinoin was commonly more responsible than antibiotics. Knowing that alterations in the microbial colonization of the flora regions may precede infectious disease and bacterial resistance, treatment options and follow-up procedures in acne vulgaris should be carefully determined to reduce the risk of destruction of the microbial flora.
Severe Acne in Female Patients Treated with Isotretinoin is associated with Dysbiosis and its Consequences
https://pdfs.semanticscholar.org/aa42/f3e7260c399337f8e74faac8f8899ccce5ee.pdf
The study included only female patients. The conclusions are therefore only relevant for females. Isotretinoin is associated with dysbiosis, malabsorption (with visceral fat decrease) and signs of dysimmunity. Symptoms develop more than 20 years after the intakeof the medication taken at usual range and duration. A facilitating role of Propionibacterium acnes cannot be excluded. Isotretinoin is known to impair stem cells renewal and TLR2 expression in the mucosa of the small gut. These pharmacological effects, explaining the efficacy of the medication on acne (the metabolic syndrome of the pilosebaceous gland) may induce the progressive atrophy of the jejunal mucosa and its long-lasting consequences. No therapy is available yet. Patients, prescribers and authorities should be aware of this adverse event which incidence is high (2.6% of outward gastroenterological consultations)especially when multi-annual surveillance for several years are expected
In addition, isotretinoin normalizes [58,59] exaggerated TLR-2- mediated responses in acne patients [60,61]. Since TLR2 plays many positive physiological roles, deleterious consequences of its blockade are expected. TLR2 regulates the production of neurotrophic factors in intestinal smooth muscle cells and promotes survival of enteric neurons and glial cells [62,63]. TLR2 controls mucosal renewal. Cells kinetics of villous columnar epithelial cells are modulated by TLR2 and controls the proliferation of indigenous bacteria [64-66]. TLR2 enables local tolerance via Bacteroides fragilis. It discriminates between pathogens and symbiotic bacterial molecules in a process that engenders commensal beneficial colonization [67,68]. TLR2 controls indigenous bacteria proliferation in the upper alimentary tract. Lack of TLR-2 contribute to the settlement of undesirable bacteria, especially Gram-positive, or candida [69,66,70,4].
Gut bacteria can stop cancer drugs from working
https://www.nature.com/news/gut-bacteria-can-stop-cancer-drugs-from-working-1.22109
Presence of particular microbes or enzymes could explain why some treatments are ineffective for certain people.
there is increasing evidence that apersons unique microbiome the population of bacteria and other microbes that live in their body can be key to determining whether or not a drug works for their condition.
Researchers now have evidence that healthy people metabolize some drugs in different ways depending on their microbial make-up.
Bacteria living in the human body will eat any nutrient that comes their way, whether its food from the hosts diet or a drug that the person is taking. But this dietary flexibility can become problematic if the microbes metabolize a drug into useless or toxic compounds.
Whether a person believes Accutane is still stored in the body or not after all these years, (I don't)
I do get the feeling from time to time that the drug is still working.
It can stop now... Right?
Interesting observation, like its swithced on something that we need to turn off
On a minor level I know my kinesiologist during treatment has picked up that certain muscles of mine havent turned off - they then know how to treat this.
I dont know enough about anatomy or our nervous system but it could be that tane has turned something on and although it has well andtruly left our bodies it has turned something on....I dont know, just a thought....
Ill ask some more questions if drugs are known to do this
I think were on the right track concerning dysregulation of the HPA Axis, more so on the glucocosteroids dysfunction within the HPA Axis, there is a strong study on this and interesting read, more importantly it says that a reset of the HPA Axis is possible with Mifespristone as they done a study on rats being administered Accutane and reversing its effects with Mifespristone.
Please read from the link below and maybe we can start from this angle with numerous studies performed how retinoic acid affects the glucocosteroids and causes the negative feedback loop to not work properly which results in HPA dyregulation, which can cause dry skin, androgen testosterone deficencies, neurotransmitter imbalances. I believe if we can get our HPA Axis to function again as it should most of our symptoms should resolve.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4030330/
3 hours ago, Ronnie99 said:I think were on the right track concerning dysregulation of the HPA Axis, more so on the glucocosteroids dysfunction within the HPA Axis, there is a strong study on this and interesting read, more importantly it says that a reset of the HPA Axis is possible with Mifespristone as they done a study on rats being administered Accutane and reversing its effects with Mifespristone.
Please read from the link below and maybe we can start from this angle with numerous studies performed how retinoic acid affects the glucocosteroids and causes the negative feedback loop to not work properly which results in HPA dyregulation, which can cause dry skin, androgen testosterone deficencies, neurotransmitter imbalances. I believe if we can get our HPA Axis to function again as it should most of our symptoms should resolve.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4030330/
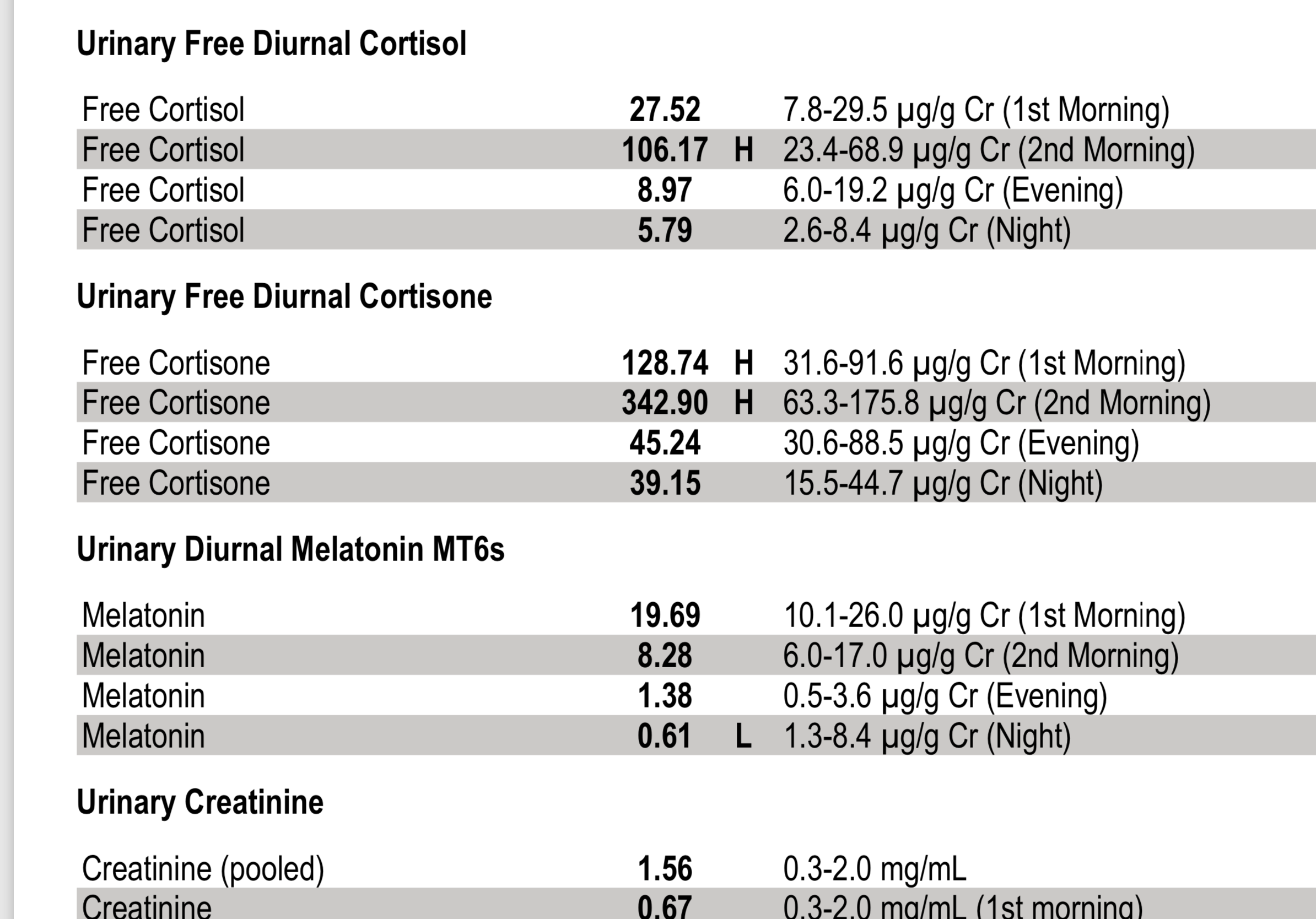
Have you had tests showing you have high cortisol?
@guitrman, Thanks.
Noticed one nasty tidbit in the first study you posted:
QuoteStaphylococcus aureus colonization was prominent in the microbial floras of nose and oropharynx and 2 of 14 nasal isolates were detected to be methicilline resistant while Escherichia coli with extended spectrum beta lactamase activity was detected in fecal floras of patients in isotretinoin group.
Something I caught in that study I posted is that they don't clearly indicate dosage. It says something along the lines of a suspension of 30mg/ml isotretinoin was given to the mice, but didn't clearly indicate dosage. This study is useless when, for all we know, the amount of isotretinoin given to the mice was inconsequential.