 Acne.org Products
Acne.org ProductsOn 01/15/2017 at 5:35 AM, Weltschmerz47 said:also, an important gene in that pathway..rs12934922 .. is messed up for me!
If youve got one T inrs12934922, I wouldnt worry. If youve got TT inrs12934922then you should get real vitamin A, but its not as significant asrs7501331..
i am TT
https://selfhacked.com/2014/12/22/importance-real-vitamin-retinol/#Alcohol_Depletes_Vitamin_A
So, mutations in that gene affect your body's ability to convert beta-carotene (precursor to vitamin A found in plants) to retinol. Lo and behold, I am a double T too. It seems that if an unfavorable mutation can exist, I will have it. This mutation is in addition to my body sucking at converting ALA (precursor found in plant foods) to EPA (essential Omega 3). These two things together may further may explain why I felt so bad on a vegan diet. And to think I once believed the vegan diet was the most healthy. Now a days, I try to eat lots of eggs, chicken, and red meat.
In regards to your awesome finding with phytol: Recently, I have tried consuming vast amounts of greens daily by cooking my own soups and frequently buying lettuce and kale. Do you think these products contain significant amounts of phytol? I'll be sure to look into hemp seeds as well. Phytol seems like a fairly scarce topic when you search online.
3 hours ago, ACCUiTy_drANE said:That's actually very useful information. Mirtazapine is essentially nothing more than an antihistamine, aside from its activity on the 5-HT2C receptor. As an inverse agonist on that site, it helps release dopamine and norepinephrine in the frontal cortex. Nortriptyline does the same thing, but has greater antidepressant qualities. Agomelatine also works on the 5-HT2C receptor (antagonist), and is a highly accessible medication. I was just pondering if I should try Agomelatine today. It seems that drugs that inhibit 5-HT2C can have potent anti-anhedonic actions for a subset of people. So perhaps you should look into those other medications if Mirtazapine helped.It's worth noting I have noticed multiple ex-Accutane and ex-SSRI sufferers praise 5-HT2C antagonist/inverse agonist agents.
When I tried it first in 2011, agomelatine felt almost as effective as melatonin for sleep, but gave a bit of a mood kick (mild though) of which melatonin didn't provide. I was going to try it again, but apparently it has quite a high incidence of liver injury compare to other ADs (example: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4407422/
I found this out when my new psych ordered LFTs as she handed me the script. This is actually recommended standard practice now instructed from the manufacturer! That put me off going back on it. Just a heads up if you consider.
On 12/9/2016 at 2:10 AM, ehohel said:Then why are like 90%> of accutane users just fine, if you know so much about this, then please enlighten me with the cure. Muchas gracias
On the contrary! Oh...believe me, nobody is fine after taking accutane. It's just a question of time. Some will see the effects just after finishing their treatment (this way it's easy to know the culprit) , others will see symptoms arise one after another, very discretely until it becomes a big issue 10, 20 years post tane. in the later case, these people doesn't realise it is connected to accutane. And if you notice, all the people that claim to be going well after tane are young.
18 hours ago, SaffronAide said:Is it possible that i may grow less because of Accutane ??
I do believe Accutane had atleast some effect on my height growth. When I started taking Accutane it was August and in the spring before that I was 175 cm and now I'm 178. The thing is that I was 12 at the moment and I always had been bigger than my peers, but now I'm slightly shorter than average young man in my country. Also I have very small hands. Feels like I didn't never fully develop into a man. I have been playing with the idea what it would be like if hopped on HGH now as a adult.
Hey guys, little update.
I am beginning TRT as of this morning. Linked below is my reasoning behind this and what pushed me to this over the past 4 years. It's quite extensive and I think.. seeing what many of you post here, you could learn a lot from.
[Edited link out]
I'll take a little step back for now, but will be sure to keep you guys updated. Thank you everyone for your help til now.
On 1/16/2017 at 10:16 PM, ehohel said:That's just one guy who suggests to go straight for the TRT. I totally believe TRT will fix your issues (as long as you stay on it) and that choice in the end is totally yours. But I'm looking for a permanent fix, not a crutch that you have to use for the rest of your life. But like I said, in the end choice is totally yours. Perhaps doing a T steroid cycle followed by PCT would work better than just regular PCT. I haven't used Anastrozole probably long enough, and I'm already off of it mostly because I really wanted to start bulking up and take Ostarine again. But so far being off anastrozole for 3 days didn't give me any rebound (perhaps too early) and a couple days ago I started ostarine which makes me sort of fatigued. But for the most part on the AI I was feeling pretty good and cheery. If anyone does go for an AI though just do small dosage, don't nuke E with 1mg/day for 2 weeks like I did. I already had shitty joints and that probably didn't help.Low dose long term would probably be the better option. I did something like 1mg ED for 2 weeks then 0.25mg EOD for like a week and a half. Once I finish my Ostarine cycle I'll go back on anastrozole low dose for maybe 2 months see how that goes.
I apologize for not getting my bloods tested after anastrozole before starting ostarine. :S
Hi, do you know what your lowest reading for estrogen has ever been?
Anyone else for that matter?
Here in the UK they do not have a lower range so even 5 pmol/L would be dismissed by GP's.
The range given is <170 pmol/L
I believe for a young male it should be at least 72 + or as a urologist kindly informed me:
A study by Finkelstein et al New England Journal of Medicine (2013;369:1011-1022) suggested that low oestradiol affected sexual function and fat distribution in younger men and many accept 95-170 pmol/l as the normal range.
In fact I will post the whole email again for anyone interested:
I really have found researching low E very difficult so if anyone is able to share any knowledge that would be really helpful.
Nelson Vergel has some strong views on E if anyone is interested.
I have warned before to not assume that E is high - you should always have a blood test.
Many thanks.
On 17.1.2017 at 7:48 PM, SaffronAide said:Guys i talked with a Accutane Victim. He is a Doctor !! thats a pretty useful coincidance..
And i learned the problem !!! listen me up !
The hidden problem is : ''The dead receptor'' theory which many of people here have already heard that. And this theory explains why we have normal hormone levels while we are having serious side effects about hormones !
He said : Accutane (which is a cancer drug) kills the hormone receptors in the body. With this , your body can produce hormones but it couldn't use it because your receptors are already dead.. Thats the simple abstract of it. Go and search this if you want to know more. But this is it.We should focus this ALL TOGETHER and solve this. Go and see your doctor please , ask them to this theory and ask them for solve , cure and explanation !
Post your informations here so we can cure ourselves. Please -in this week- go and see your doctor and get knowledge about this receptors. We have to be together , thats the only way for cure !!Reply this comment when you learned the knowledge about it , i will post my information here too.
Please..
Reply me and this post.We should share to all people and victims , we must focus on this receptor problem !
And for the gods sake can somebody please start a online signature campaign ? about Accutane so they can hear us !!
YES! definitly yes, is this the right way.
example: all my hormone level in every year after accutane are incredibly normal, test for the doctor is high but I live a post-accutane life with ED that destroy 90% of my sexual power and body.
few years ago i tried l-carnitine in high doses, famous for boost androgen-receptors. And the result were incedible, for a short period every day I had spontanous erection, sex interesting, mentally and physically strenght like pre accutane
carnitine boost momentaneus my receptors that can use hormone like a healthy body.
but maybe I overdid it with the doses, I have perhaps had a crash and stopped working.
"your body can produce hormones but it couldn't use it" yes all damages from accutane are summarized in this perfect sentence
On 1/19/2017 at 3:38 AM, hatetane said:Hi, do you know what your lowest reading for estrogen has ever been?
Anyone else for that matter?
Here in the UK they do not have a lower range so even 5 pmol/L would be dismissed by GP's.
The range given is <170 pmol/L
I believe for a young male it should be at least 72 + or as a urologist kindly informed me:A study by Finkelstein et alNew England Journal of Medicine(2013;369:1011-1022) suggested that low oestradiol affected sexual function and fat distribution in younger men and many accept 95-170 pmol/l as the normal range.
In fact I will post the whole email again for anyone interested:The issue is how we deal with a probable drug induced side effect, similar to what we see with antidepressants and finasteride where effects can last for years afterwards. Do we wait for the body to recover with time or do we give more medication to reverse these changes (given that these problems are rare)?Giving Sildenafil (daily Cialis better) is quite reasonable , as the penis needs regular oxygenation and deterioration occurs if morning erections are lost. There are no risks with this.Low Oestradiol increases the risk of osteoporosis in the long term and should not be ignored.Treating him would involve "unlicensed" medication. Clomid would increase both T and Oestradiol and potentiate recovery of the pituitary, but opinions would differ as there are no trials or guidelines to help us here. Some doctors today feel totally restrained by guidelines.I really have found researching low E very difficult so if anyone is able to share any knowledge that would be really helpful.
Nelson Vergel has some strong views on E if anyone is interested.
I have warned before to not assume that E is high - you should always have a blood test.
Many thanks.
[Edited image out]
that's my only estrogen test, that's following about a month of DIM + IC3.
On 1/18/2017 at 11:23 PM, Kynarr said:Hey guys, little update.
I am beginning TRT as of this morning. Linked below is my reasoning behind this and what pushed me to this over the past 4 years. It's quite extensive and I think.. seeing what many of you post here, you could learn a lot from.
[Edited link out]I'll take a little step back for now, but will be sure to keep you guys updated. Thank you everyone for your help til now.
I do like that guys reasoning. I'm sure you'll feel a hellva lot better on TRT but please let us know if there's any interaction with the other side effects that don't seem to correlate with T. (bowel issues, inflammation, etc;)
About to run a trial of this stuff. Not hoping for much more of just why not. I'll let you know how it all goes.
https://www.ncbi.nlm.nih.gov/pubmed/22666519
On 1/19/2017 at 6:41 AM, ehohel said:About to run a trial of this stuff. Not hoping for much more of just why not. I'll let you know how it all goes.
where are you getting it from , and how much are you taking?
[Edited link out]
[Edited link out]
Acute or chronic inflammation induces a net increase of total copper in blood, synovial fluid and inflamed areas, mobilized from endogenous stores [13]. Chronic inflammation may lead to depletion of copper stores, implying the need for exogenous copper supply in order to effectively cope with the inflammatory pathologies. While copper complexes are commonly administered by injection, the AI activity of subcutaneous administration of copper complexes in animals was also shown to be proportional to total amount of copper injected [34].
The present study indicates that topical administration of copper in form of the tripeptide may offer an effective alternative to injection. Since a realistic dimension for topical application of GHK-Cu as patch may cover 10cm2of skin, based on our results 2.33mg of copper would become available over 48h. This may be compared to a subcutaneous injection of 300mg/kg of copper aspirinate in rats without adverse effects, while it proved effective in treating experimental subplantar edema even at a dose of 10mg/kg.
I am just about done with life at this point. I am so depressed at this point in time. Oh great.... its 2017. I have tried Paleo, Raw, Vegan, Fasting, Frutarian, and just plain balance of unproccessed foods.. doesnt matter... This acid burned every gland and receptor in my body to where i feel like a sad robot.
I really dont have much to say, I just dont feel like i signed up for this powerful of a medication.
7 years post accutane now, and it keeps getting worse and worse.
On 1/19/2017 at 7:16 AM, tryingtohelp2014 said:where are you getting it from , and how much are you taking?
[Edited link out]
[Edited link out]
Acute or chronic inflammation induces a net increase of total copper in blood, synovial fluid and inflamed areas, mobilized from endogenous stores [13]. Chronic inflammation may lead to depletion of copper stores, implying the need for exogenous copper supply in order to effectively cope with the inflammatory pathologies. While copper complexes are commonly administered by injection, the AI activity of subcutaneous administration of copper complexes in animals was also shown to be proportional to total amount of copper injected [34].
The present study indicates that topical administration of copper in form of the tripeptide may offer an effective alternative to injection. Since a realistic dimension for topical application of GHK-Cu as patch may cover 10cm2of skin, based on our results 2.33mg of copper would become available over 48h. This may be compared to a subcutaneous injection of 300mg/kg of copper aspirinate in rats without adverse effects, while it proved effective in treating experimental subplantar edema even at a dose of 10mg/kg.
Getting it from ceretropic, they just added it to their site today.
I'm not going for topical, I already have needles and such so just going to do subQ injections. Going to do 1mg first dose, 2mg next and adjust as if I deem necessary. I haven't found tons of info for dosage, I think I saw somewhere on longecity of someone doing 4mg subQ per day? I'll look more into dosage when it arrives on friday/saturday.
" Chronic inflammation may lead to depletion of copper stores "
Probably explains why I'm borderline deficient in copper haha.
On 1/19/2017 at 6:02 AM, ehohel said:[Edited image out]
that's my only estrogen test, that's following about a month of DIM + IC3. I do like that guys reasoning. I'm sure you'll feel a hellva lot better on TRT but please let us know if there's any interaction with the other side effects that don't seem to correlate with T. (bowel issues, inflammation, etc;)
Thanks. Your E is about perfect, right? Dim will have decreased it i guess. What;s your T like?
On 1/19/2017 at 7:54 AM, hatetane said:On 1/19/2017 at 6:02 AM, ehohel said:[Edited image out]that's my only estrogen test, that's following about a month of DIM + IC3. I do like that guys reasoning. I'm sure you'll feel a hellva lot better on TRT but please let us know if there's any interaction with the other side effects that don't seem to correlate with T. (bowel issues, inflammation, etc;)
Thanks. Your E is about perfect, right? Dim will have decreased it i guess. What;s your T like?
[Edited image out]
2 hours ago, ehohel said:About to run a trial of this stuff. Not hoping for much more of just why not. I'll let you know how it all goes.
Well, I can't say I blame you. Like you, I follow Ceretropic's product line closely. On one hand, it seems we have nothing to lose by trying all these peptides, but on the other hand, I sort of feel like it's not necessarily productive to pump any peptide they release in my body. The reason I hesitate is because many of these compounds may be useless unless injected on a long-term basis. And depending on the compound we're talking about and the amount of time administered, vital restorative mechanisms can potentially be downregulated. Then there are the horror stories of some peptides (i.e., P21) causing a persistent autoimmune response, and several anecdotes of people incurring low-grade immune reactions from it. That's enough for me to steer clear. But I'll give these two new compounds a look. Who knows. I hope for the best for you. It seems you have made progress with what you have tried already.
39 minutes ago, ACCUiTy_drANE said:Well, I can't say I blame you. Like you, I follow Ceretropic's product line closely. On one hand, it seems we have nothing to lose by trying all these peptides, but on the other hand, I sort of feel like it's not necessarily productive to pump any peptide they release in my body. The reason I hesitate is because many of these compounds may be useless unless injected on a long-term basis. And depending on the compound we're talking about and the amount of time administered, vital restorative mechanisms can potentially be downregulated. Then there are the horror stories of some peptides (i.e., P21) causing a persistent autoimmune response, and several anecdotes of people incurring low-grade immune reactions from it. That's enough for me to steer clear. But I'll give these two new compounds a look. Who knows. I hope for the best for you. It seems you have made progress with what you have tried already.
I took the risk with p21 cause of an anecdote claiming it reversed their amphetamine induced stutter. And I am having excellent results regarding that. It hasn't totally stopped mine, but my stutter is minimal now after a full vial of p21 I may give the nasal spray a try in the future, but like you said I should probably see if I can get tests for CNTF antibodies.
They do have a bunch of other peptides not available to public that I have access to that I haven't been trying. (like half of them have to do with GH). But these newest two, especially the GHK-CU has me really interested.
I'm having excellent digestion progress regarding BPC-157. GHK-CU also has tons of healing properties, also lots specifically gut related so perhaps this will be a score.
My biggest let down was the like $600 I dumped into epitalon. Slightly more restful sleep wasn't worth that much in my book. 
Given that I'm using a SARM, my single biggest issue right now has gotta be inflammation, joint pain, and tendonitis like symptoms. Perhaps for this I should just get to a doctor... How much I miss being a on cortisol steroid and not feeling a spec of pain. I probably caused tons of damage due to my physically demanding job while I wasn't able to gain muscle, thus putting massive strain on my joints possibly even permanent damage. Given how much success AI has given me, after my SARM cycle I'm going to probably do a PCT involving SERM, followed by low dose AI. If that doesn't fix my T, I'll do what Kynarr did and just do TRT, it really isn't worth all this extra stress when there is a temporary solution until we can actually figure out a real permanent solution (if there is one).
On 17 janvier 2017 at 10:29 PM, ehohel said:Previously my stomach wasn't working basically at all. I eat food, and sometime later I'll shit, that's it. No signs of digestion (even though it was probably still happening). But now I'm getting gas, burping
I'm sorry but this sounds like nonsense. Eating and shitting later with nothing in between is what it is supposed to be, that way my digestion worked when I was kid. Getting gas and burping would indicate some problems, on contrary.
22 hours ago, IntimateHemp said:I am just about done with life at this point. I am so depressed at this point in time. Oh great.... its 2017. I have tried Paleo, Raw, Vegan, Fasting, Frutarian, and just plain balance of unproccessed foods.. doesnt matter... This acid burned every gland and receptor in my body to where i feel like a sad robot.
I really dont have much to say, I just dont feel like i signed up for this powerful of a medication.
7 years post accutane now, and it keeps getting worse and worse.
Please be a patience! Don't hurt yourself or give up. You are yust really depresed, I'm going to psychotherapy and i fell just better but no so much good . Actually my will is very poor but i m a fight man and never stop to strugle... Did anyone of you guys notice how milk who has a lot of vitamins A has a really bad influence on us in generally like digestive , fell like a poison.!!
16 hours ago, ehohel said:I took the risk with p21 cause of an anecdote claiming it reversed their amphetamine induced stutter. And I am having excellent results regarding that. It hasn't totally stopped mine, but my stutter is minimal now after a full vial of p21 I may give the nasal spray a try in the future, but like you said I should probably see if I can get tests for CNTF antibodies.They do have a bunch of other peptides not available to public that I have access to that I haven't been trying. (like half of them have to do with GH). But these newest two, especially the GHK-CU has me really interested.
I'm having excellent digestion progress regarding BPC-157. GHK-CU also has tons of healing properties, also lots specifically gut related so perhaps this will be a score.
My biggest let down was the like $600 I dumped into epitalon. Slightly more restful sleep wasn't worth that much in my book.
Given that I'm using a SARM, my single biggest issue right now has gotta be inflammation, joint pain, and tendonitis like symptoms. Perhaps for this I should just get to a doctor... How much I miss being a on cortisol steroid and not feeling a spec of pain. I probably caused tons of damage due to my physically demanding job while I wasn't able to gain muscle, thus putting massive strain on my joints possibly even permanent damage. Given how much success AI has given me, after my SARM cycle I'm going to probably do a PCT involving SERM, followed by low dose AI. If that doesn't fix my T, I'll do what Kynarr did and just do TRT, it really isn't worth all this extra stress when there is a temporary solution until we can actually figure out a real permanent solution (if there is one).
same symptoms , same blood tests over and over. my recent one from last week... same depressed copper again
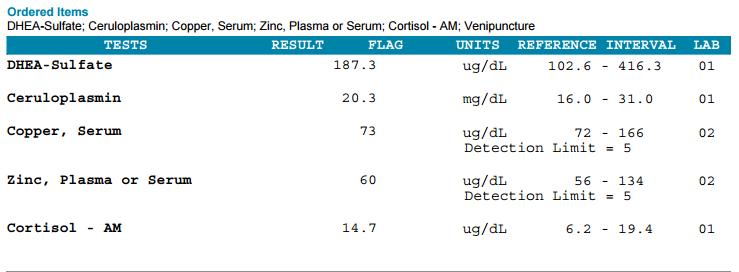
https://www.ncbi.nlm.nih.gov/pubmed/3679695
Modification of vitamin A metabolism in rats fed a copper-deficient diet.
Abstract
The liver is the main storage site of vitamin A and copper. Inverse relationships between copper and vitamin A liver concentrations have been suggested. We have investigated the consequences of a copper-deficient diet on liver and blood vitamin A storage in Wistar rats. Animals were fed either a copper-deficient diet for 45 days from weaning, or an identical diet containing adequate amounts of copper. Concentrations of vitamin A were determined by isocratic high performance liquid chromatography using UV detection. We have observed in the liver of the rats fed a copper-deficient diet a significantly higher mean level of retinyl esters (148 +/- 37 micrograms/g of liver) and retinol (3.3 +/- 1.4 micrograms/g of liver) compared to the mean concentration of the retinyl esters (53 +/- 8.5 micrograms/g of liver) (p less than 0.01) and retinol (1.4 +/- 0.5 micrograms/g of liver) (p less than 0.01) in controls. Opposite results were observed in the serum of the group fed a copper-deficient diet as these rats had a significantly lower level of retinol (22 +/- 4 micrograms/100 ml) compared to the mean concentration in the controls (64 +/- 20 micrograms/100 ml) (p less than 0.01). These findings suggest that a copper-deficient diet may cause defective transport of vitamin A from liver to blood. This experimental model may be useful to further investigate unusual liver vitamin A and copper concentrations observed in children during various hepatobiliary diseases.
17 hours ago, IntimateHemp said:I am just about done with life at this point. I am so depressed at this point in time. Oh great.... its 2017. I have tried Paleo, Raw, Vegan, Fasting, Frutarian, and just plain balance of unproccessed foods.. doesnt matter... This acid burned every gland and receptor in my body to where i feel like a sad robot.
I really dont have much to say, I just dont feel like i signed up for this powerful of a medication.
7 years post accutane now, and it keeps getting worse and worse.
I eat all fruit too, not even vegetables all raw. When you say you tried fasting, what kind? Dry fasting/water fasting? how long? Was you taking anything while doing the fasting? Please be honest with yourself... Ecig, toothpaste, smoking, it all counts...
On 18/01/2017 at 5:48 AM, SaffronAide said:Guys i talked with a Accutane Victim. He is a Doctor !! thats a pretty useful coincidance..
And i learned the problem !!! listen me up !
The hidden problem is : ''The dead receptor'' theory which many of people here have already heard that. And this theory explains why we have normal hormone levels while we are having serious side effects about hormones !
He said : Accutane (which is a cancer drug) kills the hormone receptors in the body. With this , your body can produce hormones but it couldn't use it because your receptors are already dead.. Thats the simple abstract of it. Go and search this if you want to know more. But this is it.We should focus this ALL TOGETHER and solve this. Go and see your doctor please , ask them to this theory and ask them for solve , cure and explanation !
Post your informations here so we can cure ourselves. Please -in this week- go and see your doctor and get knowledge about this receptors. We have to be together , thats the only way for cure !!Reply this comment when you learned the knowledge about it , i will post my information here too.
Please..
Reply me and this post.We should share to all people and victims , we must focus on this receptor problem !
And for the gods sake can somebody please start a online signature campaign ? about Accutane so they can hear us !!
Yeah and what did he say next???
You spoke to a Dr, he said to fix receptors - how did he fix his???
3 hours ago, TrueJustice said:Yeah and what did he say next???
You spoke to a Dr, he said to fix receptors - how did he fix his???
If the problem is truly with "dead receptors" or desensitized receptors, the first place my mind goes is in the realm of hormesis. The basic idea is: A compound may cause a harmful effect in a small dose, but when microdosed, a compensatory ("good") mechanism may take place. The best analogy is Naltrexone. For those who don't know: We know this drug antagonizes (i.e., blocks) opioid receptors. That's all it does at 50 mg. But at small doses (4.5 mg and lower), it blocks the receptors for a short time, which causes the body to compensate by 1) up-regulating opioid receptors, 2) sensitizing the receptors, and 3) boosting endorphins. So a small dose does something radically different than a big dose.
So could a compound do something similar for androgen receptors? If we blocked these receptors with microdoses of some compound, perhaps something similar could occur with androgen receptors. It's not impossible, given the fact there are myriad real-world examples of hormesis at work. The problem is doing so safely and NOT accidentally making the problem worse. The blockage would have to be short-lived so that the body could respond by sensitizing receptors. And that's assuming testosterone/DHT is the root of our issues in the first place! As a side note, I know I've heard people mention microdosing Propecia and Accutane to deal with persistent side effects. What a repugnant thought though. 
https://www.ncbi.nlm.nih.gov/pubmed/27138887
8 minutes ago, ACCUiTy_drANE said:If the problem is truly with "dead receptors" or desensitized receptors, the first place my mind goes is in the realm of hormesis. The basic idea is: A compound may cause a harmful effect in a small dose, but when microdosed, a compensatory ("good") mechanism may take place. The best analogy is Naltrexone. For those who don't know: We know this drug antagonizes (i.e., blocks) opioid receptors. That's all it does at 50 mg. But at small doses (4.5 mg and lower), it blocks the receptors for a short time, which causes the body to compensate by 1) up-regulating opioid receptors, 2) sensitizing the receptors, and 3) boosting endorphins. So a small dose does something radically different than a big dose.So could a compound do something similar for androgen receptors? If we blocked these receptors with microdoses of some compound, perhaps something similar could occur with androgen receptors. It's not impossible, given the fact there are myriad real-world examples of hormesis at work. The problem is doing so safely and NOT accidentally making the problem worse. The blockage would have to be short-lived so that the body could respond by sensitizing receptors. And that's assuming testosterone/DHT is the root of our issues in the first place! As a side note, I know I've heard people mention microdosing Propecia and Accutane to deal with persistent side effects. What a repugnant thought though.
Too lazy to google right now, but are there any existing drugs that's a 5ar antagonist with short half life?
Flutamide is a non-steroidal AR antagonist with a half-life of only 8 hours.
Spironolactone is an AR antagonist, with active metabolites having a half-life of 13-16 hours.
.