 Acne.org Products
Acne.org ProductsI am very new to this community. I have been reading and learning a lot of new things which I wish had done prior to procedure done to face.
I visited my local derm in first week of January for acne scars. She suggested a acne scar revision process that would basically help my scars rise (which now I think she meant subcision) and PRP. I went to her office next week with PRP of my blood.
After the procedure, my face was swollen and bruised for at least 4-5 days. I have developed 2 noticable bumps of right cheek. I asked her about those she said she filled deeper scars with plasma/growth rate of my blood. They will settle down eventually. Last week when I visited her she said, it's an error in filling. They will eventually resolve automatically.
Can someone please help me know if that's a known complication? I need to decide further course of action.
8 hours ago, PRPhelp said:I went to her office next week with PRP of my blood.
Wait...what? You spunyour own blood? Like the doctor doesn't have a centrifuge in her office?
PRP is basically plasma protein derived from white blood after the red blood cells are removed. IT GETS ABSORBED BY THE SKIN IN ABOUT 24 HOURS AND IT CANNOT BE USED AS A FILLER.
8 hours ago, PRPhelp said:I have developed 2 noticable bumps of left cheek. I asked her about those she said she filled deeper scars with plasma/growth rate of my blood. They will settle down eventually. Last week when I visited her she said, it's an error in filling. They will eventually resolve automatically.
This is most likely from subcision and not from PRP. Hypertrophic scarring can occur when there is a damage to the reticular dermis (eg. deeper layer).
6 hours ago, Sirius Lee said:Wait...what? You spun your own blood? Like the doctor doesn't have a centrifuge in her office?
PRP is basically plasma protein derived from white blood after the red blood cells are removed. IT GETS ABSORBED BY THE SKIN IN ABOUT 24 HOURS AND IT CANNOT BE USED AS A FILLER.
Yes I had to get those samples from another lab
6 hours ago, Sirius Lee said:This is most likely from subcision and not from PRP. Hypertrophic scarring can occur when there is a damage to the reticular dermis (eg. deeper layer).
This is scary..Can you please help me know how these can be treated.

The procedure also resulted in PIH, which is being treated with cream containing hydroquinone(4pc) + tretinoin(0.05) + mometasone furoate combination.
I am observing facial har growth and swelling after using it.
Any other ways PIH can be treated?
A doctor said that to treat PIH for ethnic skin, you can use a combination of Azelaic Acid, Kojic Acid, Niacinamide, Vitamin C (Ascorbic Acid), Alpha Arbutin. She said Hydroquinone and lasers can worsen PIH for people of ethnic backgrounds.
I've had PIH gradually go away. I've also had it not go away and TCA peels helped. Hydroquinone 4% didn't help me and it aggravated my skin. But this is me.
14 hours ago, PRPhelp said:Yes I had to get those samples from another lab
This is scary..Can you please help me know how these can be treated.
The procedure also resulted in PIH, which is being treated with cream containing hydroquinone(4pc) + tretinoin(0.05) + mometasone furoate combination.
I am observing facial har growth and swelling after using it.
Any other ways PIH can be treated?
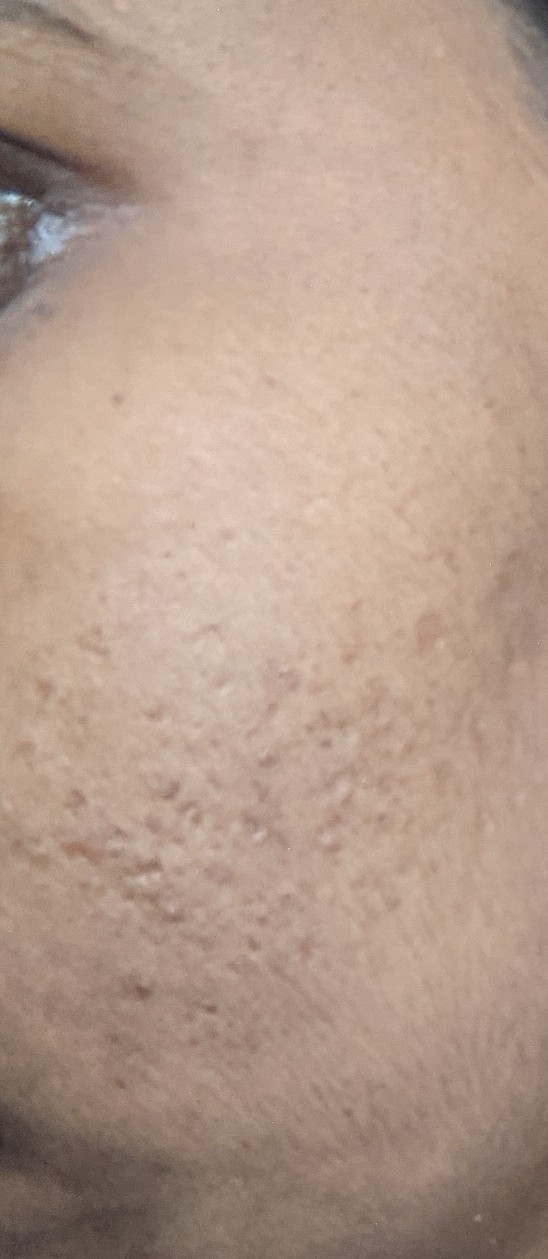
Are these the entry points on the picture ?
16 hours ago, PRPhelp said:This is scary..Can you please help me know how these can be treated.
I can only offer you the textbook solution for keloid/hypertrophic scar.
Intralesional verapamil, fluorouracil, bleomycin, and interferon alfa-2b injections appear to be beneficial for treatment of established keloids.
Keloid formation often can be prevented if anticipated with immediate silicone elastomer sheeting, taping to reduce skin tension, or corticosteroid injections. Once established, however, keloids are difficult to treat, with a high recurrence rate regardless of therapy. Evidence supports silicone sheeting, pressure dressings, and corticosteroid injections as first-line treatments. Cryotherapy may be useful, but should be reserved for smaller lesions. Surgical removal of keloids poses a high recurrence risk unless combined with one or several of these standard therapies. Alternative postsurgical options for refractory scars include pulsed dye laser, radiation, and possibly imiquimod cream.
On 2/23/2021 at 2:20 AM, Sirius Lee said:I can only offer you the textbook solution for keloid/hypertrophic scar.
Intralesional verapamil, fluorouracil, bleomycin, and interferon alfa-2b injections appear to be beneficial for treatment of established keloids.
Keloid formation often can be prevented if anticipated with immediate silicone elastomer sheeting, taping to reduce skin tension, or corticosteroid injections. Once established, however, keloids are difficult to treat, with a high recurrence rate regardless of therapy. Evidence supports silicone sheeting, pressure dressings, and corticosteroid injections as first-line treatments. Cryotherapy may be useful, but should be reserved for smaller lesions. Surgical removal of keloids poses a high recurrence risk unless combined with one or several of these standard therapies. Alternative postsurgical options for refractory scars include pulsed dye laser, radiation, and possibly imiquimod cream.
So as it turns out the procedure was punch elevation. I can't find much data on it online.
I don't understand why these excessive extrusions are caused. Will they settle down on their own?

On 2/23/2021 at 2:20 AM, Sirius Lee said:I can only offer you the textbook solution for keloid/hypertrophic scar.
Intralesional verapamil, fluorouracil, bleomycin, and interferon alfa-2b injections appear to be beneficial for treatment of established keloids.
Keloid formation often can be prevented if anticipated with immediate silicone elastomer sheeting, taping to reduce skin tension, or corticosteroid injections. Once established, however, keloids are difficult to treat, with a high recurrence rate regardless of therapy. Evidence supports silicone sheeting, pressure dressings, and corticosteroid injections as first-line treatments. Cryotherapy may be useful, but should be reserved for smaller lesions. Surgical removal of keloids poses a high recurrence risk unless combined with one or several of these standard therapies. Alternative postsurgical options for refractory scars include pulsed dye laser, radiation, and possibly imiquimod cream.
The other cheek looks comparatively okay. At least no visible excessive extrusions.

8 hours ago, PRPhelp said:So as it turns out the procedure was punch elevation. I can't find much data on it online.
I don't understand why these excessive extrusions are caused. Will they settle down on their own?
You mean the doctor never clearly communicated to you that you will be getting punch excision? That sounds troubling. Is she a board-certified dermatologist or plastic surgeon? Do you mind sharing the name with us?
On a brighter note, these are still relatively fresh scars, so it's possible that they can go down on their own. To expedite it, you can start with silicone sheets to flatten them. However, if that doesn't work, you will need something more stronger like cortisone injection.