 Acne.org Products
Acne.org Products@ColinbokoYour hormone levels are in great standing. What are your Accutane sides? Do you workout? What's your diet like? Is gaining muscle difficult? ED? How much accutane did you take? Do you have a result of your methylation and detox pathways through a dna test? How old are you? Please provide clear, detailed data.
On 3/13/2018 at 12:04 AM, flynn said:Would be useful to know your main symptoms, do you even have sexual dysfunction from Accutane?.
I'm no doctor so take everything I say with a pinch of salt (I could be completely wrong).
- High DHEA-S fits the profile
- Normal/high LH is normal/healthy
- High FSH is unusual (doesn't fit with my theory - so either theory is wrong or you are an anomaly).There could be any number of reasons for high FSH, you may just naturally produce more FSH then most people. But I would advise maybe getting it checked out.
One possibility (really don't mean or want to scare you here) - Normal Testosterone, normal LH and high FSH can indicate spermatogenic failure. You should look into semen analysis. Again though, this could just be a complete random level. Which indicates nothing.
Could you or I post the results on forum with blood test so we can start to analyse all the blood tests? - [removed]
I do have sexual dysfunction. Basically no libido, cant keep it up etc.
The thing that worries me is although my testosterone looks good and all, I never had it checked before accutane.... So like what if it did drop and I have no idea..... Another strange thing is my DHT is kinda low, estradiol seems pretty high. No idea what to make of this
18 hours ago, Frage said:I'm concerned that the only way we would be able to get such treatment in a timely manner is if we did it ourselves. And not only the time factor, but companies currently charge hundreds of thousands of dollars for crispr treatments. I'm desperate enough, but I'm not all that confident in my abilities. Then again I haven't done shit in 3 weeks, just wallowing in hopeless depression. And I have heard its relatively easy, whatever that means. What could go wrong? Give myself cancer? Don't even know if I view that as a bad thing anymore. BumpEdit: We also still need more information about what genes to target based on a bit more exact thoughts on what enzymes/androgens/receptors are not functioning correctly.
You may be right, but look online. People are already experimenting on themsleves with CRISPR and related technologies (high inadvisable right now). But I imagine its only a matter of time before that technology becomes incredibly cheap and easy to use. Just as you can buy research compounds online now and take them. I bet you'll be able to buy something similar in the near future. You already can buy 5AR1 and 5AR2 CRISPR gene activator online (but they wont work in neurons) and you need a delivery system (hard part) but the possibility is there and its very very real. Believe me, if I think one of these therapies becomes available and has a chance, I'll be the first to buy it online and test it on myself. Then you can decide if you want to take the risk.
10 minutes ago, Kynarr said:@ColinbokoYour hormone levels are in great standing. What are your Accutane sides? Do you workout? What's your diet like? Is gaining muscle difficult? ED? How much accutane did you take? Do you have a result of your methylation and detox pathways through a dna test? How old are you? Please provide clear, detailed data.
Raging fatigue even after sleeping 10+ hours
Cognitive/memory troubles (but long term memory is fine)
Cold/Heat intolerance
Telogen effluvium body wide
Dry red eyes (pressure behind them and in forehead)
Rarely getting sick
low libido
rarely get morning wood
Muscle wasting
Crazy weight gain in mid section/face
Atrophy of my vocal cord muscles
1 hour ago, Colinboko said:Raging fatigue even after sleeping 10+ hours
Cognitive/memory troubles (but long term memory is fine)
Cold/Heat intolerance
Telogen effluvium body wide
Dry red eyes (pressure behind them and in forehead)
Rarely getting sick
low libido
rarely get morning wood
Muscle wasting
Crazy weight gain in mid section/face
Atrophy of my vocal cord muscles
Interesting.
For well over a year, I have been running on the belief that many of us have androgen issues. I have myself begun TRT in Feb 2017, and overall many sides have improved since. As your hormones are already good, nobody in their right mind would ever recommend that you start a hormone treatment.
I'm not sure why then, you suffer so many sides which resemble so closely an androgen deficiency. Maybe then it's not so much low hormone levels, but a desensitization? Food for thought.
I lack info on you, and I don't know what you do to keep yourself healthy, but since TRT is not an option for you, then I believe the best course of action, if you're not already doing it, is to live an optimal lifestyle, ie; workout, meditate, eat a healthy paleo/bulletproof diet, fast from time to time, take supplements.
Here's maybe an easy supplements sample list as I've myself been taking. Forego the Enanthate in your case ")
1 hour ago, Kynarr said:Interesting.For well over a year, I have been running on the belief that many of us have androgen issues. I have myself begun TRT in Feb 2017, and overall many sides have improved since. As your hormones are already good, nobody in their right mind would ever recommend that you start a hormone treatment.
I'm not sure why then, you suffer so many sides which resemble so closely an androgen deficiency. Maybe then it's not so much low hormone levels, but a desensitization? Food for thought.
I lack info on you, and I don't know what you do to keep yourself healthy, but since TRT is not an option for you, then I believe the best course of action, if you're not already doing it, is to live an optimal lifestyle, ie; workout, meditate, eat a healthy paleo/bulletproof diet, fast from time to time, take supplements.
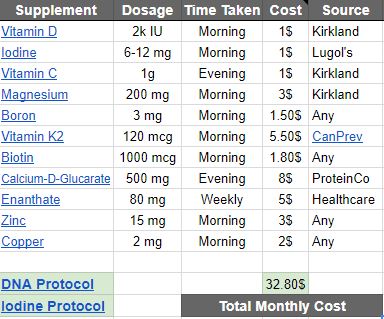
Here's maybe an easy supplements sample list as I've myself been taking. Forego the Enanthate in your case
Supplement Dosage Time Taken Vitamin D 2k IU Morning Iodine 6-12 mg Morning Vitamin C 1g Evening Magnesium 200 mg Morning Boron 3 mg Morning Vitamin K2 120 mcg Morning Biotin 1000 mcg Morning Calcium-D-Glucarate 500 mg Evening Enanthate 80 mg Weekly Zinc 15 mg Morning Copper 2 mg Morning
I™m thinking more along the lines of some form of adrenal issue. Planning on getting my cortisol tested soon. Also, my estradiol is pretty high
High DHEA in attempt to heighten cortisol ? I don™t know. I™m puzzled.
Not entirely sure it™s a desensitization because I grow a beard relatively fast. Chest hair. The whole works.
On 3/13/2018 at 2:10 AM, Kynarr said:I'm not sure why then, you suffer so many sides which resemble so closely an androgen deficiency. Maybe then it's not so much low hormone levels, but a desensitization? Food for thought.
I don't think it's a desensitization in relation to receptors etc. I think its a failure to translate the testosterone signal into an appropriate response as DHT and other neurosteroids are depleted as in PFS, due to a reduction in expression/activity of 5AR. If you care to read, I have explained in depth here. See what you think - [removed]
On 3/13/2018 at 2:15 AM, Colinboko said:High DHEA in attempt to heighten cortisol ? I dont know. Im puzzled.
Not entirely sure its a desensitization because I grow a beard relatively fast. Chest hair. The whole works.
High DHEA-S is confusing and common. Accutane has been shown to downregulate expression of the 3B-HSD type 1 enzyme by 6 fold in the skin (this could have happened in other areas of the body as well). Guess what one of the roles of 3B-HSD is? It converts DHEA to androstenedione. Could Accutane have downregulated 3B-HSD type 1 around the body, leading to a build up DHEA-S as less of it is being converted to androstenedione?
Again I've talked about this stuff in depth on this post - [removed]
On 3/13/2018 at 4:41 AM, flynn said:See what you think - [removed]
I dont think this stops at hormones to be honest with you.
People have chased this for so many years.
Peripheral Nervous System Involved in Post-Finasteride Syndrome Patients with Severe Erectile Dysfunction, New Study Demonstrates for the First Time
[Edited link out]
The nervous system might be affected. This is true. I have a blood test to prove it.
All of the blood tests done on these patients though have been conflicting when you look at what PFS sufferers are posting.
Just like Accutane.
People have high Testosterone, low Testosterone, high dhea, normal dhea, low dhea, high estrogen, low estrogen, normal estrogen. Now you have high fsh, low fsh.
Something going on might be taking hormones for a ride,
but they are not necessarily doing the driving.
Im looking at regulators of steroidogenic enzymes.
I'd like to chime in on the whole 5AR theory and give my two cents.
ive been doing steroid blasts (recreationally to get big) and I can for sure point out that there are times where it's as if my hormones do not "work" and it's a lot more apparent when you're injecting 500mg test e a week. Then there are "flare ups" where it's noticeably working and I'm stronger. I believe I've noticed that my tendinitis flares up whenever my hormones do work. I've takenmelanotan 2 and if I recall correctly it made my hormones consistently work while taking it. I never really noticed as I was taking it that it was because of that but I'll test again soon. I read somewhere on Reddit in the steroids forum about someone pointing out thatmelanotan 2 makes their steroids much much more effective that's when I sorta pieced together that. But I need to test again to be sure, now that I'm aware.
These are the potential side effects of brain damage. Many display a number of these symptoms. It wouldn't be a far cry to say nearly all symptoms displayed here branch from the symptoms of brain damage (ie. Lipid levels being affected by the systemic metabolic dysregulation and neuroendocrine due to the brain changescaused by accutane)
Traumatic brain injury: a disease process, not an event.
https://www.ncbi.nlm.nih.gov/m/pubmed/20504161/
Traumatic brain injury (TBI) is seen by the insurance industry and many health care providers as an "event." Once treated and provided with a brief period of rehabilitation, the perception exists that patients with a TBI require little further treatment and face no lasting effects on the central nervous system or other organ systems. In fact, TBI is a chronic disease process, one that fits the World Health Organization definition as having one or more of the following characteristics: it is permanent, caused by non-reversible pathological alterations, requires special training of the patient for rehabilitation, and/or may require a long period of observation, supervision, or care. TBI increases long-term mortality and reduces life expectancy. It is associated with increased incidences of seizures, sleep disorders, neurodegenerative diseases, neuroendocrine dysregulation, and psychiatric diseases, as well as non-neurological disorders such as sexual dysfunction, bladder and bowel incontinence, and systemic metabolic dysregulation that may arise and/or persist for months to years post-injury. The purpose of this article is to encourage the classification of TBI as the beginning of an ongoing, perhaps lifelong process, that impacts multiple organ systems and may be disease causative and accelerative. Our intent is not to discourage patients with TBI or their families and caregivers, but rather to emphasize that TBI should be managed as a chronic disease and defined as such by health care and insurance providers. Furthermore, if the chronic nature of TBI is recognized by government and private funding agencies, research can be directed at discovering therapies that may interrupt the disease processes months or even years after the initiating event.
With no further ado, here is the evidence that accutane causes brain damage.
Dermatologists' attitudes, prescription, and counseling patterns for isotretinoin: a questionnaire-based study.
http://www.ncbi.nlm.nih.gov/pubmed/25689814
"A 25-question survey was emailed to 7,013 dermatologists included in a proprietary database (MBD, Inc.) and anonymous responses were collected. 591 board-certified dermatologists participated. Thirty-seven percent of the responding dermatologists believe that isotretinoin may cause psychiatric disturbances. Dermatologists' opinions on this relationship did not significantly impact prescription practices in patients with history of depression (P=0.056) or in patients being treated with an antidepressant (P=0.118)."
Functional brain imaging alterations in acne patients treated with isotretinoin.
http://www.ncbi.nlm.nih.gov/pubmed/15863802
"RESULTS: Isotretinoin but not antibiotic treatment was associated with decreased brain metabolism in the orbitofrontal cortex (-21% change versus 2% change for antibiotic), a brain area known to mediate symptoms of depression.
Conclusion: This study suggests that isotretinoin treatment is associated with changes in brain functioning."
A 4-month treatment trial with isotretinoin was associated with a decrease in brain functioning in the orbito-frontal cortex, a brain region implicated in depression.
13-cis Retinoic acid (accutane) suppresses hippocampal cell survival in mice.
http://www.ncbi.nlm.nih.gov/pubmed/15251924
We now show, in a mouse model, that endogenous RA generated by synthetic enzymes in the meninges acts on hippocampal granule neurons, and chronic (3-week) exposure to a clinical dose of 13-cis RA may result in hippocampal cell loss.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC387382/
"This report demonstrates that a clinical dose (1 mg/kg/day) of 13-cis-RA in mice significantly reduces cell proliferation in the hippocampus and the subventricular zone, suppresses hippocampal neurogenesis, and severely disrupts capacity to learn a spatial radial maze task. The results demonstrate that the regions of the adult brain where cell proliferation is ongoing are highly sensitive to disruption by a clinical dose of 13-cis-RA."
Retinoic Acid and Affective Disorders: The Evidence for an Association
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3276716/
"Increased concentrations of homocysteine have also been associated with attacks of violent anger. Isotretinoin administration to human subjects was shown to be associated with increased concentrations of homocysteine, as well as decreases in 5-methyl-tetrahydrofolate, providing a potential metabolic mechanism by which isotretinoin may promote depression."
"In the case of patients reported to the Norwegian Medicines Agency, single photon emission computed tomography (SPECT) of the brain was performed in 15 cases who reported lasting neurological symptoms. Altered brain function was seen in all cases involving altered or reduced frontal lobe blood flow. Ten of these patients were evaluated to have organic brain damage."
13-Cis-retinoic acid decreases hypothalamic cell number in vitro.
https://www.ncbi.nlm.nih.gov/pubmed/20708044 "13-Cis-retinoic acid (13-cis-RA) causes depression-related behavior in mice. Hypothalamic dysregulation has been implicated in clinical depression. In fact, apoptosis of hypothalamic neurons may lead to depression after myocardial infarction. . . .We hypothesize that the ability of 13-cis-RA to decrease hypothalamic cell number may contribute to the increased depression-related behaviors observed in mice."
Anyway, at the risk of offending those who are not as lucky as I have been, I want to mention thatI have made a full recoveryfrom accutane (or as close to 100% as I can expect), using the safe and pretty cheap(<$300 for 3 months) protocol I outlinein here https://docs.google.com/document/d/1gGkP_NQ8tmYkOADlG2VuEX17YvQJKgnfcEtgy5_6y7c/edit# .
I don't get brain fog or social anxiety anymore, my hormones are back in check, ED isgone, but I do have performance anxiety left from bad experiences when it was still there, but I think it is improving steadily. Scars and injuries I picked up when I took Accutane never healed as well, but now I can rehab and manage them a lot easier.
Sorry if you try it and it doesn't as much as it helped me. That said, its all based on research and so it should still help a fair bit regardless, even if you don't get back to 100%
Quick question guys...
The free and total testosterone test I ordered was recommended for women and prepubescent boys.
Im just wondering if a 22 year old man should have ordered it. It was something like an LC/MS method? I didnt realize the exact details on this test until I reviewed it on quest diagnostics. Can you guys give me some insight on this?
7 hours ago, Fchawk said:These are the potential side effects of brain damage. Many display a number of these symptoms. It wouldn't be a far cry to say nearly all symptoms displayed here branch from the symptoms of brain damage (ie. Lipid levels being affected by the systemic metabolic dysregulation and neuroendocrine due to the brain changescaused by accutane)
Dermatologists' attitudes, prescription, and counseling patterns for isotretinoin: a questionnaire-based study.
Agreed, the brain damage theory is a possible cause/reason. Again sorry for all the long posts. I do have a few things to say about this though:
1. When these studies look at changes in brain metabolism/activity/blood flow. They find changes/persistent changes. Is this surprising? We know that there are persistent changes to the activity of our own neural pathways such as the dopaminergic reward pathway. We all know ourselves that major pathways in the brain aren't working as they once were (they are no longer being activated). Which factors in the brain do you think alter metabolism/activity/blood flow? Surely the activity of major neural pathways by neurotransmitters like Dopamine plays a pretty significant role in determining the metabolism/activity/blood flow of a brain region. I mean ultimately this is the core function of the brain. Do you really think that if we managed to fix this and find a way to reactivate these pathways through through whatever the cure ends up working, that you wouldn't see a large increase in brain metabolism/activity/blood flow in specific regions of the brain as well?
2. Just to reinstate, studies looking at blood flow. Dopamine is a vasodilator. Activity of pathways will effect the blood flow to regions of the brain. The orbitofrontal cortex receives dopaminergic signals. What I'm saying is, there may be altered blood flow now. But if you were able to reactivate the right pathways, we may see a recovery of some of that blood flow/activity.
3. For the sexual dysfunction symptoms: People have reported experiencing recovery or partial recovery of the sexual function (libido etc.) for brief or long periods. If the sexual dysfunction side effect was caused by permanent brain damage, how could anyone ever experience any significant improvement in these symptoms. Surely if the pathway has been damaged/destroyed, it will not longer work. Additionally, people have reported periods of losing sex drive/libido for a week on Accutane for it then to return. This makes no sense in light of brain damage.
4. I'll grant you that Accutane damages the hippocampus whilst you are on it. But this still doesn't explain sexual dysfunction and this doesn't mean that neurogenesis (and the damage) in the hippocampus can't necessarily be recovered overtime by substance/supplements which stimulate hippocampal neurogenesis.
5 hours ago, Iamme. said:majority of my blood tests came back fine, doctor still cannot explain pressure from behind my right eye/blocked right sinus. MRI booked in for a week from now.
I have the exact same symptoms in the same area. Very interested to know what /if they find anything.
8 hours ago, mikez said:I have the exact same symptoms in the same area. Very interested to know what /if they find anything.
Worst case scenario. The progression.
Blood flow. Nerve Damage. Muscle Damage.
Ischemic optic neuropathy is damage of the optic nerve caused by a blockage of its blood supply.
The scary thing is some of this starts to get into the Realm of MS.
sometimes optic neuritis is a precursor to development of MS, so if you have optic neuritis, your doctor may recommend an MRI. If imaging shows "white matter" lesions indicating damage to myelin in nerve fibers, there is a 56 percent chance of developing MS within 10 years. But even with normal results, a person with optic neuritis has a 22 percent chance of developing MS.
Maybe it's just some sinus pressure.
Id make sure you see that mri report.
17 hours ago, Fchawk said:These are the potential side effects of brain damage. Many display a number of these symptoms. It wouldn't be a far cry to say nearly all symptoms displayed here branch from the symptoms of brain damage (ie. Lipid levels being affected by the systemic metabolic dysregulation and neuroendocrine due to the brain changescaused by accutane)
Traumatic brain injury: a disease process, not an event.
https://www.ncbi.nlm.nih.gov/m/pubmed/20504161/
Traumatic brain injury (TBI) is seen by the insurance industry and many health care providers as an "event." Once treated and provided with a brief period of rehabilitation, the perception exists that patients with a TBI require little further treatment and face no lasting effects on the central nervous system or other organ systems. In fact, TBI is a chronic disease process, one that fits the World Health Organization definition as having one or more of the following characteristics: it is permanent, caused by non-reversible pathological alterations, requires special training of the patient for rehabilitation, and/or may require a long period of observation, supervision, or care. TBI increases long-term mortality and reduces life expectancy. It is associated with increased incidences of seizures, sleep disorders, neurodegenerative diseases, neuroendocrine dysregulation, and psychiatric diseases, as well as non-neurological disorders such as sexual dysfunction, bladder and bowel incontinence, and systemic metabolic dysregulation that may arise and/or persist for months to years post-injury. The purpose of this article is to encourage the classification of TBI as the beginning of an ongoing, perhaps lifelong process, that impacts multiple organ systems and may be disease causative and accelerative. Our intent is not to discourage patients with TBI or their families and caregivers, but rather to emphasize that TBI should be managed as a chronic disease and defined as such by health care and insurance providers. Furthermore, if the chronic nature of TBI is recognized by government and private funding agencies, research can be directed at discovering therapies that may interrupt the disease processes months or even years after the initiating event.
With no further ado, here is the evidence that accutane causes brain damage.
Dermatologists' attitudes, prescription, and counseling patterns for isotretinoin: a questionnaire-based study.
http://www.ncbi.nlm.nih.gov/pubmed/25689814
"A 25-question survey was emailed to 7,013 dermatologists included in a proprietary database (MBD, Inc.) and anonymous responses were collected. 591 board-certified dermatologists participated. Thirty-seven percent of the responding dermatologists believe that isotretinoin may cause psychiatric disturbances. Dermatologists' opinions on this relationship did not significantly impact prescription practices in patients with history of depression (P=0.056) or in patients being treated with an antidepressant (P=0.118)."
Functional brain imaging alterations in acne patients treated with isotretinoin.
http://www.ncbi.nlm.nih.gov/pubmed/15863802
"RESULTS: Isotretinoin but not antibiotic treatment was associated with decreased brain metabolism in the orbitofrontal cortex (-21% change versus 2% change for antibiotic), a brain area known to mediate symptoms of depression.
Conclusion: This study suggests that isotretinoin treatment is associated with changes in brain functioning."
A 4-month treatment trial with isotretinoin was associated with a decrease in brain functioning in the orbito-frontal cortex, a brain region implicated in depression.
13-cis Retinoic acid (accutane) suppresses hippocampal cell survival in mice.
http://www.ncbi.nlm.nih.gov/pubmed/15251924
We now show, in a mouse model, that endogenous RA generated by synthetic enzymes in the meninges acts on hippocampal granule neurons, and chronic (3-week) exposure to a clinical dose of 13-cis RA may result in hippocampal cell loss.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC387382/
"This report demonstrates that a clinical dose (1 mg/kg/day) of 13-cis-RA in mice significantly reduces cell proliferation in the hippocampus and the subventricular zone, suppresses hippocampal neurogenesis, and severely disrupts capacity to learn a spatial radial maze task. The results demonstrate that the regions of the adult brain where cell proliferation is ongoing are highly sensitive to disruption by a clinical dose of 13-cis-RA."
Retinoic Acid and Affective Disorders: The Evidence for an Association
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3276716/
"Increased concentrations of homocysteine have also been associated with attacks of violent anger. Isotretinoin administration to human subjects was shown to be associated with increased concentrations of homocysteine, as well as decreases in 5-methyl-tetrahydrofolate, providing a potential metabolic mechanism by which isotretinoin may promote depression."
"In the case of patients reported to the Norwegian Medicines Agency, single photon emission computed tomography (SPECT) of the brain was performed in 15 cases who reported lasting neurological symptoms. Altered brain function was seen in all cases involving altered or reduced frontal lobe blood flow. Ten of these patients were evaluated to have organic brain damage."
13-Cis-retinoic acid decreases hypothalamic cell number in vitro.
https://www.ncbi.nlm.nih.gov/pubmed/20708044 "13-Cis-retinoic acid (13-cis-RA) causes depression-related behavior in mice. Hypothalamic dysregulation has been implicated in clinical depression. In fact, apoptosis of hypothalamic neurons may lead to depression after myocardial infarction. . . .We hypothesize that the ability of 13-cis-RA to decrease hypothalamic cell number may contribute to the increased depression-related behaviors observed in mice."
Anyway, at the risk of offending those who are not as lucky as I have been, I want to mention thatI have made a full recoveryfrom accutane (or as close to 100% as I can expect), using the safe and pretty cheap(<$300 for 3 months) protocol I outlinein here https://docs.google.com/document/d/1gGkP_NQ8tmYkOADlG2VuEX17YvQJKgnfcEtgy5_6y7c/edit# .
I don't get brain fog or social anxiety anymore, my hormones are back in check, ED isgone, but I do have performance anxiety left from bad experiences when it was still there, but I think it is improving steadily. Scars and injuries I picked up when I took Accutane never healed as well, but now I can rehab and manage them a lot easier.Sorry if you try it and it doesn't as much as it helped me. That said, its all based on research and so it should still help a fair bit regardless, even if you don't get back to 100%
Sorry which part of the protocol addresses the severe chronic fatigue many of us suffer from?
We spend a shit load of time talking about sexual sides and depression ( myself included) for good reason as we want to cure these issues but what about the chronic fatigue that most have going on simultaneously??
You could fix the sexual issues but if youre still out of your mind with fatigue youre going to continue to be unhappy!!
20 minutes ago, TrueJustice said:Sorry which part of the protocol addresses the severe chronic fatigue many of us suffer from?We spend a shit load of time talking about sexual sides and depression ( myself included) for good reason as we want to cure these issues but what about the chronic fatigue that most have going on simultaneously??
You could fix the sexual issues but if youre still out of your mind with fatigue youre going to continue to be unhappy!!
Im forced to believe the chronic fatigue is related to cortisol. Do you also wake up early for no reason? And do you have super light sleep? My fatigue is easily one of the worst symptoms. Have you had cortisol tested? I have crazy high DHEA-s forcing me to believe Im in one of the last stages of adrenal burnout. Because Im ALWAYS exhausted
15 minutes ago, Colinboko said:40 minutes ago, TrueJustice said:Sorry which part of the protocol addresses the severe chronic fatigue many of us suffer from?We spend a shit load of time talking about sexual sides and depression ( myself included) for good reason as we want to cure these issues but what about the chronic fatigue that most have going on simultaneously??
You could fix the sexual issues but if youre still out of your mind with fatigue youre going to continue to be unhappy!!
Im forced to believe the chronic fatigue is related to cortisol. Do you also wake up early for no reason? And do you have super light sleep? My fatigue is easily one of the worst symptoms. Have you had cortisol tested? I have crazy high DHEA-s forcing me to believe Im in one of the last stages of adrenal burnout. Because Im ALWAYS exhausted
You and I are very similar based on what we post, very similar!!
I believe Ive tested but as usual nothing definitive with results.
Ive taken adrenal supplements before but no real relief, wouldnt hurt to take again I suppose.
Yeah that lite sleep is horrendous- the best sleep I ever get are those afternoon naps when you have no work commitments etc,
that would be on the weekend I suppose.
Waking up feeling refreshed hasnt happened in years, I mean 15 years - no joke.
44 minutes ago, TrueJustice said:You and I are very similar based on what we post, very similar!!I believe Ive tested but as usual nothing definitive with results.
Ive taken adrenal supplements before but no real relief, wouldnt hurt to take again I suppose.
Yeah that lite sleep is horrendous- the best sleep I ever get are those afternoon naps when you have no work commitments etc,
that would be on the weekend I suppose.
Waking up feeling refreshed hasnt happened in years, I mean 15 years - no joke.
Literally same. I find I actually feel better when I get LESS sleep. Like some process is happening during my sleep to make me feel like such crap when I wake up. Like either the low cortisol is causing low blood sugar (I could see this being possible because I always wake up with dry hands, mouth etc. which is a common trend with low bs). Or its something immune related that is activated when Im asleep and causes me to feel like crap upon waking up.
Adrenal supplements wont do a thing. If its true adrenal burnout (essentially Addisons disease) we would need hydrocortisone to feel relief again.
On 3/14/2018 at 5:44 AM, Colinboko said:Have you had cortisol tested?
I would go right back to walkinlab and order the am cortisol test then.
You are now in the unfortunate game that many have played for years.
Including myself.
Everyone thinks they know what it is, until its not. (I do still believe in the possibility of some "it" factors that have a trickle down effect.)
There is some evidence though, you can also look at @Babisposts, one of his diagnosis involved the pituitary.
The effect of different doses of isotretinoin on pituitary hormones.
https://www.ncbi.nlm.nih.gov/pubmed/25721216
but again this is just a different hormone, same scenario like I just posted.
You'll find ranges all over the board post accutane.
[Edited link out]
Clayton, did you test your estrogen as well?
My results show an elevated cortisol level (yours is almost at maximum also), and a high estrogen.
Do you suffer from hair loss?
Very surprised to see high DHT, as my understanding is this would be very low?
@flynn@Dubya_BThere is this as well.
Vitamin A Increases DHT By Enhancing 5-alpha Reductase
http://www.ncbi.nlm.nih.gov/pubmed/10423178
Administration of all-trans-retinoic acid (ATRA; 60 mg/kg daily for 3 days) to male rats increased the rate of 5alpha-dihydrotestosterone (5alpha-DHT) formation from testosterone in microsomal fractions in vitro. The formation of androstane-3alpha,17beta-diol from testosterone was also increased because of the higher concentration of 5alpha-DHT produced in microsomal incubations.
it was found that administration of ATRA to gonadectomized male rats produced complete feminization of the enzyme.
What is the main androgen produced by the testes? Testosterone.
These findings suggest that ATRA is a novel positive regulator of the 5alpha-reductasethat in combination with the removal of circulating androgen, which normally suppresses 5alpha-reductase levels, feminizes the expression of this enzyme in rat liver
Urban Dictionary: mindfuck
an idea or concept that shakes one's previously held beliefs or assumptions about the nature of reality.
1 hour ago, Colinboko said:Literally same. I find I actually feel better when I get LESS sleep. Like some process is happening during my sleep to make me feel like such crap when I wake up. Like either the low cortisol is causing low blood sugar (I could see this being possible because I always wake up with dry hands, mouth etc. which is a common trend with low bs). Or its something immune related that is activated when Im asleep and causes me to feel like crap upon waking up.Adrenal supplements wont do a thing. If its true adrenal burnout (essentially Addisons disease) we would need hydrocortisone to feel relief again.
Agree - aside from the placebo effect I still sleep like shit and still have crap energy every other day.
Cortisol testing - Im gonna say save yourself the money, like every other test....its high, its low....whatever, Dr just give me the fucking cure already....
Think this way, assume its high, than what?? go take supplements only to find you feel no different in the same way adrenal supplements are ineffective.
About sexual dysfunction:
I reported a while ago I did many tests and reached a few conclusions.
First of all, I experienced depression 1 year AFTER the treatment ended (8 months in 2011). The depression lasted from 2012 to 2014 at least.
While the depression has completely vanished the low libido has remained. I remember back in June 9, 2012 I was 100% different from what I am today (had an erection in public) and was probably experiencing high libido. Over the years the whole thing evolved to a point I (for the first time in 2 decades) stopped with masturbation for months and between 2016-17 spend more than a year without it.
Nowadays I don't have any sexual needs, so no interest in:
- Women
- Sex
- FAP
At all. I could spend the next 20 years without any of those things and there are no recurring thoughts in my mind about any of this. I am interested in women, however light years from the way I was acting before.
And when I decide to masturbate the pleasure isn't in any way comparable to 5-10 years ago.
My take on this:
- Accutane is responsible at least 60% in what changed in my body and mind.
- My lifestyle and the way I was brought up (what I always thought about these things, my life experiences...) account for the remaining 40%.
Things are not going to change substantially, but they will improve. In this I believe.
What were the results that caught my attention?
1) Prolactin levels. This is perhaps the most important.
4 tests showed results between 20-28. For a man the ideal levels are below 10. So measure your PRL, which is the best indication if you are impotent. In my case these levels (even that high) do not justify taking Cabergoline, which if I am not mistaken would require years and there's always a chance of the problem coming back once treatment is stopped. Also it's a very expensive drug (and the same can be said about testosterone replacement therapy).
- There's a study from 2014 saying that TRT (or taking dopamine agonists) didn't help with sexual dysfunction from Accutane (don't take these seriously since I never see blood test results from the victims). And I don't recommend TRT since it has some nasty side effects like shrunken testicles (not to mention it's an artificial way of increasing testosterone. And we don't want to force this kind of change in our bodies, messing with them even more, do we?).
It has been suggested that vitamin B-6 + vitamin-E and other supplements can increase libido and decrease prolactin. The problem with that idea is that the EFSA recommends no more than 25 mg/day (even 50 can have side effects) and a few sources say you need to increase that to 50-200. I am not going to do that.
http://lmgtfy.com/?q=vitamin+B-6+decrease+prolactin
You can read the EFSA tolerable upper intake levels for vitamins here:
http://www.efsa.europa.eu/sites/default/files/efsa_rep/blobserver_assets/ndatolerableuil.pdf
Not surprisingly the max intake for vitamin D is the same I was taking the 1st time, when my TT increased from 307 to 419.
2) Total and free testosterone + vitamin D. My first result before taking vitamin D-3 was 307. After 3 months taking D-3 (7000 IU - 2 pills, once a week) = 419 (total testosterone increased), and decreased to 357 after another 3 months reducing the dose to 1 pill. (Free test 6.15 the first time, then 6.91 and 7.21)
At the same time vitamin D-3 levels were 26 in the first test. I rarely go outside, and when I do I cover my body with long sleeves and use sunscreen protector. After supplementing = 40. The last tests I did showed the levels were still at 40.
Ideal levels are I believe 50-60.
This link says the following:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1472884/
"Although the normal range for serum testosterone might vary between different laboratories, the normal range for early morning testosterone in male adults is approximately 300 ng/dL to 1000 ng/dL. An early morning total serum testosterone level of less than 300 ng/dL clearly indicates hypogonadism, and under most circumstances benefit will be derived from testosterone replacement therapy. A healthy male adult patient with a serum testosterone level greater than 400 ng/dL is unlikely to be testosterone deficient, and therefore clinical judgment should be exercised if he has symptoms suggestive of testosterone deficiency."
That means I don't have hypogonadism, and also managed to improve things and after some changes in my lifestyle.
What I am going to do is to stop using sunscreen protector since I only go outside for a few minutes a day (in the morning, when we can expose our skin without risks) and this + taking vitamin D-3 (which may also be needed in the winter, if the Sun isn't 50 degrees above the horizon *) will help increasing both TT (and free) + vitamin D.
* See this article: https://articles.mercola.com/sites/articles/archive/2012/03/26/maximizing-vitamin-d-exposure.aspx
3) LH and FSH. That NCBI article says:
"Primary hypogonadism is associated with low levels of testosterone and high-normal to high levels of LH and FSH. Secondary hypogonadism is associated with low levels of testosterone and normal to low levels of LH and FSH."
"In selected patients, FSH, LH, and prolactin can be measured. If the FSH and LH levels are raised, this suggests a primary testicular cause, and if levels are low or normal, a hypothalamic or pituitary cause should be considered. A raised prolactin level suggests that further investigation of the pituitary gland should be undertaken"
My LH result was 4,61 mUI/mL (lab ranges 1,24 - 8,62 MUI/ML);
FSH 6,54 mUI/mL (lab ranges 1,27 - 19,26 MUI/ML).
There's nothing wrong with my testicles based on the above explanation (my levels are normal).
And the MRI from the sella turcica showed nothing abnormal. Which also rules out (if I am not mistaken) the need for "a further investigation of the pituitary gland". I also did two more tests worth mentioning:
4) Spermogram/semen analysis.
5) Abdominal ultrasonography.
Also got normal results.
All the other blood tests showed no inconsistencies and were within lab ranges.
For example:
DHT (Dihydrotestosterone) = 360 pg/mL (lab ranges for men 31-40 years old (33 in my case) = 17,7 - 775,0 pg/mL
DHEA-S = 262 mcg/dL (lab ranges for men 31-40 years old = 106 - 464 mcg/dL
Not to mention zinc, vitamin B-12, TSH, free T4 and others.
With all that said, here's what I suggest and am actually doing (besides testing myself again months from now):
- A complete overhaul in the diet. This is even more important than going to the gym. Go to someone (not just any doctor) that specializes in this area, and, of course, say to him that adjusting your testosterone and PRL levels is the main objective.
- Do the same thing for your workout routine with a PERSONAL TRAINER. Since it's said that in order to increase testosterone we need to exercise intensely there's a need not only to change this, also to add supplements like Whey Protein, creatine, fish oil, etc. that can help boosting your health.
- Try to avoid everything else that is said to impact these levels. A few examples from a podcast I always listen to:
- http://naturopathicearth.com/2017/11/20/npe75-deodarant/
- http://naturopathicearth.com/2017/07/26/phthalates/
- http://naturopathicearth.com/2017/07/05/npe-radio-plastics/
https://academic.oup.com/jcem/article/99/11/4346/2836774
https://www.medscape.com/viewarticle/830137
https://prostate.net/articles/bisphenol-a-bpa-and-phthalates-linked-to-sexual-problems-in-men
There's a lot of things that someone can do that hasn't been covered. I would include from him the episodes about screen addiction, fluoride, EMF radiation.. And since I mentioned screen addiction, use blue blocker lenses to sleep better (less eye fatigue). Also check these tips on bias lightning: https://goo.gl/gPU1mk (for me relevant because I spend a considerable time studying in my iPAD).
What all this has to do with sexual dysfunction? Everything accounts for the "rest". It's not just Accutane that contributed to my current state.
And I'll do everything possible to improve my health, more than ever before. The more that happens the more I'll know if these changes can mitigate or nullify this side effect from Accutane.
Always remember this bit from Wikipedia:
- Isotretinoin is also associated with sexual side effects, namely erectile dysfunction and reduced libido. In October 2017, the UK MHRA issued a Drug Safety Update to physicians in response to reports of these problems.
This was in response to an EU review, published in August 2017, which states that a plausible physiological explanation of these side effects "may be a reduction in plasma testosterone".
The review also stated that "the product information should be updated to include sexual dysfunction including erectile dysfunction and decreased libido as an undesirable effect with an unknown frequency".
There have also been reports of spermatogenesis disorders, such as oligospermia. 27 cases of sexual dysfunction report either negative dechallenge or positive dechallenge.
**
What Dr. Pezzi said about vitamin B-6:
***************************************************
***************************************************
***************************************************
******************************************************
High doses of vitamin B 6 can improve libido by reducing prolactin secretion in both sexes. B 6 can also improve the quality and intensity of sexual pleasure in some people who have poor genital sensation. An average dose for these applications is 25 mg three times daily. Vitamin B 6 is excreted soon after absorption, so it is preferable to take a smaller dose of B 6 three times daily rather than one large dose. Taking too much B 6 can cause insomnia and overly vivid dream recall, so if those side effects develop you should reduce your dose or at least reduce your supplementary intake later in the day.
Doses over 200 mg daily can result in neurological disorders if taken for several months. These disorders include a loss of position and vibration sense in the legs, and sensory ataxia (incoordination due to loss of proprioception, which is joint position sensation) which worsens when the eyes are closed. Recovery from this condition is slow and may be incomplete, so it is important to avoid potentially toxic levels of B 6 . If you take fairly high amounts of B 6 , you and your doctor should be on the lookout for any early signs of toxicity.
In males, B 6 supplementation has a greater effect in stimulating libido than in women. Vitamin B 6 contributes to an increased serotonin level in specific sites in the brain (thus explaining the apparent contradiction between this and the fact that a global increase in serotonin impairs libido), which in turn causes a down-regulation of type 2A serotonin receptors (5-HT 2A receptors).
Particularly in males, lower numbers of 5-HT 2A receptors are associated with increased libido. In some men, this increase in libido can be dramatic. The downside of this is that the effect is rather transient, lasting for a week or less.
Normalizing B 6 intake for several weeks can restore some of the potential for a male to libidinally respond to future high dose B 6 regimens. However, the greatest bang for the buck (no pun intended) will be obtained during the first few times it is consumed. By the way, if you try this do not look for an immediate boost in your libidoit typically takes 3 to 5 days for an effect to be manifested.
Why doesnt B 6 cause a sustained boost in libido? One explanation is that pyridoxal 5'-phosphate (PLP), the biologically active form of vitamin B 6 , affects steroid-induced gene expression. A study * performed at the University of North Carolina at Chapel Hill found that PLP decreased transcriptional (gene) responses to androgens (e.g., testosterone), estrogens, progesterone, and glucocorticoid (e.g., cortisol) hormones.
In contrast, cells deficient in B 6 were more responsive to steroid hormones. This might suggest that the way to build bigger muscles or improve libido is to dutifully avoid B 6 since a B 6 deficiency would heighten the androgen response. However, things arent that simple since B 6 also decreased the response to some hormones, such as estrogen, that tend to counteract the effects of testosterone.
* Modulation of steroid receptor-mediated gene expression by vitamin B 6 . Tully DB, Allgood VE, Cidlowski JA. FASEB J 1994 Mar 1;8(3):343-9.
Furthermore, B 6 has a number of other effects in the body, many of which are conducive to sex and pleasure. For example, dopamine (a neurotransmitter involved in the perception of pleasure) is synthesized using a PLP-dependent enzyme.
With so many variables and so many ways to hash the data, its more helpful to focus on what people experience when they take B 6 . The bottom line is that B 6 can temporarily stimulate libido in some people. Failure to respond to B 6 might indicate that an individual manifested less suppression of estrogens than androgens, that their initial prolactin level was not sufficient to dampen libido, or several other things. Complex stuff? You bet, but the take-home message is clear: B 6 might stimulate libido. If it works, do not take high-dose supplements of it continuously for that purpose; the dose previously mentioned (25 mg three times daily) is a high-dose regimen that is considerably above the recommended daily allowance of about 2 mg.
Men who are deficient in vitamin B 6 sometimes notice a significant increase in their flaccid penile size when their deficiency is corrected. The reason for this may seem obscure but, as we will explore later in this book, vitamin B 6 can reduce the homocysteine level. Since homocysteine interferes with the production of nitric oxide (NO), and nitric oxide influences penile blood flow, it is easy to understand the link between vitamin B 6 and penile size. Correcting a B 6 deficiency can increase the size and stiffness of erections, too, but stiffness will increase more than size. **
** To understand why stiffness increases more than size, try the following experiment, or just follow along conceptually. Take a 6-inch length of an old bicycle inner tube and seal it off on one end (the inner tube is hydraulically similar to the fibrous capsule that envelopes the penis), then blow some air into the other end. You will notice that the inner tube will be floppy until it is almost full of air (in this experiment, air is analogous to blood). Once the tube is almost full, adding just a bit more air can make the tube noticeably stiffer and harder, but the size of the tube does not increase by much.
The size of the penis in its flaccid state may seem like a trivial matter, but its not. If you respond to supplementation with B 6 (or B 12 or folic acid, which well discuss later in the book), that might be a tip-off to a deficiency you might not otherwise notice. Because vitamins B 6 , B 12 , and folic acid play important roles in homocysteine metabolism and homocysteine influences your risk of cardiovascular disease, anything that alerts you to such a deficiency is worth its weight in gold. If you think that an average doctor has even the slightest clue as to the adequacy of your B 6 , B 12 , and folic acid levels, youre overestimating the competency of most doctors.
My brother developed profound weakness and numbness, and four physicians (two ER, one family practitioner, and even a neurologist) told him he had carpal tunnel syndrome in spite of the fact that his signs and symptoms were not consistent with carpal tunnel disease. In reality, his problem was due to a deficiency of vitamin B 12 that caused his spinal cord to degenerate like a piece of Swiss cheesehardly a problem that doctors should overlook or pass off as carpal tunnel syndrome.
Even if your diet contains a normal amount of vitamin B 6 , a deficiency may develop due to malabsorption, hyperthyroidism, diabetes, excessive loss, alcoholism, smoking, or the use of various drugs (e.g., corticosteroids [anti-inflammatory steroids], penicillamine, isoniazid, cycloserine, hydralazine, and some anticonvulsants). Studies in the 1960s and 1970s suggested that more B 6 is needed by women taking estrogen or oral contraceptives, but the latest research did not show any particular benefit for women taking those drugs.
******************************************************
***************************************************
***************************************************
******************************************************
"But giving more testosterone is not the remedy because elevated serum prolactin levels also prevent the body from responding normally to testosterone."
This was posted here:
[Edited link out]
In other words we need to focuse on the two. And my tests proved how true this statement is: my testosterone levels were increased, yet my PRL stayed practically the same. It can also change with ease, depending on our current condition prior to the blood test, for example our stress levels or if we have been sleeping properly. These factors can easily increase prolactin.