I recently read an article on mTOR inhibition. This article is very detailed but could possibly steer people in the wrong direction. I'll put a link to it, and add some thoughts as well.
mTOR, which stands for mammalian target of rapamycin, is an intermediate in all the factors you need to worry about: cell growth, cell proliferation, cell motility, cell survival, protein synthesis, and transcription. Healthy functioning mTOR allows your body to be anabolic and growing, and this extends to skin cells, and how specific foods can have compounded activation of mTOR with other chemicals that ignite sebaceous biosynthesis.
Knowing more about mTOR and how it interacts both inside the cell and outside the cell is very important, including cell signaling of different growth factors (like IGF-1, which is a buzzword for you guys).
Both benzoyl peroxide and isotretinoin have mechanisms for inhibiting mTOR, which can reduce cell proliferation and decrease sebum production. This can help explain why they can be effective at preventing acne and comedogenesis (see: mTORC1 and Comedogenesis).
The interesting part about this article is that it ties in many ideas that everyone here likes to talk about: how to reduce proliferation of keratinocytes and how to reduce production of skin oil. However, it's only hyperproliferation of any of these things we really need to prevent. Being healthily anabolic and growing is good. The opposite of that is of course, dying.
And what's more, hyperproliferation of sebocytes with bad lipid composition and cell proliferation in combination with systemic inflammation is the bad part. What you really need to focus on to prevent your body from growing unhealthily and from overriding and upregulating growth factors in the process is understanding what a healthy dose of anabolism is, and it all starts in the context of a low inflammatory diet (that should be obvious).
On a final note, some foods you should not be consuming, and they run in same theme of this article:
Oleic acid (olive oil) or peanut oil. These have a tendency to shut off inflammatory markers. I know what you're thinking: good right? Wrong. Some inflammatory markers help with a hormonal cascade of your body's own defenses against the original cause of inflammation. Hopefully more research will be put out on foods that aren't necessarily anti-inflammatory, but override inflammatory signals that your body intentionally has. There is a difference. If you're wondering: oleic acid and peanut oil specifically override inflammatory intermediates that allow insulin to work again. So you're body is trying to prevent more insulin production, and these oils help kick up that process again. Instead you should be focusing on the foods that ignited that inflammation in the first place and eliminating them.
Do not consume long-lasting insulinotropic foods with a high glycemic load. This would be the difference between white and brown rice: white rice is high glycemic, so it spikes insulin and insulin drops fairly quickly. Brown rice has a high load of carbs that will be digested for quite a while, keeping insulin high for extended periods of time. If you're worried about reactive hypoglycemia, women generally have a good ability of regulating blood sugar through slow release of glycogen, so this most likely this will not happen. Intaking some fat can help if men are more concerned.
Low-glycemic load while being low on the index is not really a problem, because the carb count is so low. So vegetables are OK.
Following these two recommendations and you're eliminating lots of vegetable oils and less-refined carbs like wheat bread, brown rice, beans, etc. These eliminations also do another number of beneficial things to the body I need not mention, as everyone with eyes and who's read in the nutrition section should know about.
http://www.landesbio..._full_text=true
That paper is an excellent summary of all the known factors involved in acne formation and most of the research into cause and intervention from big pharma like isotretinoin, BP and metformin to EGCG and resveraterol. And of course diet, especially the western diet.
And I wish to point out that it cites over one hundred scientific studies into these factors and how nutrients and diet habits affect those factors and thus acne. And yet people keep claiming there's no scientific evidence that diet affects acne. I guess it's like climate change deniers. No amount of evidence will change their minds.
Also funny, CBS this morning is on right now and the guests are just now talking about how inflammation is he root of disease. I see this all the time on tv and in articles in publications aimed at the general public. So why isn't the public getting it? Why isn't anti inflammatory diets the number one medical intervention?
In all honesty, I've avoided looking at this thread until now because I thought it was about "motor inhibition." I was like, "I don't have any problem moving around, so I'm not gonna check out the thread." Well, I'm glad I did look at the thread, and excuse me for being an ignoramus, because I think the whole post is great. I've become increasingly more interested in cell proliferation, sebum production and hyperkeritinization- what causes it and how to reduce it. I've been using olive oil a lot lately- maybe I'll cut it out for a bit. Thanks for the info!
That paper is an excellent summary of all the known factors involved in acne formation and most of the research into cause and intervention from big pharma like isotretinoin, BP and metformin to EGCG and resveraterol. And of course diet, especially the western diet.
And I wish to point out that it cites over one hundred scientific studies into these factors and how nutrients and diet habits affect those factors and thus acne. And yet people keep claiming there's no scientific evidence that diet affects acne. I guess it's like climate change deniers. No amount of evidence will change their minds.
Also funny, CBS this morning is on right now and the guests are just now talking about how inflammation is he root of disease. I see this all the time on tv and in articles in publications aimed at the general public. So why isn't the public getting it? Why isn't anti inflammatory diets the number one medical intervention?
Thanks for replying  I see I made a couple typos and just fixed that too.
I see I made a couple typos and just fixed that too.
mTOR is a very big intermediate that connects why benzoyl peroxide can work and why dairy could be bad for you. Can you think of anything else that can mechanistically connect those two? Of course I'm distilling those two things for this context but you get the idea.
Oleic acid can also be bad if you're really trying to develop HEALTHY cells. The oil you eat provides fatty acids to be incorporated in the phospholipids of the cell's lipid bilayer. The fluidity of the membrane's "mosaic" kind of structure is crucial for your cell to interact with its environment, and if you know anything about protein transport or protein translocation (those are 2 different things), it all makes sense. Olive oil can make your membranes "stiff." You want more saturated fats and a healthy 3:6 balance of omegas.
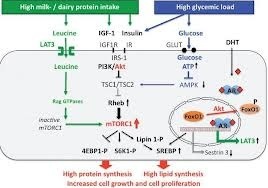
I've been trying to research into this topic more specifically in terms of sebocytes, but I'm reeeally busy. I'm hoping others can post links to mTOR. For now, check out the graphic from the research paper!
Following these two recommendations and you're eliminating lots of vegetable oils and less-refined carbs like wheat bread, brown rice, beans, etc.
Why would you want to eliminate beans? Beans generally have very low glycemic load.
From http://www.health.harvard.edu/newsweek/Glycemic_index_and_glycemic_load_for_100_foods.htm
A serving of soy beans has a glycemic load of 1. A serving of chickpeas is 3. Lentil is 5.
Potential role of FoxO1 and mTORC1 in the pathogenesis of Western diet-induced acne.
Acne in adolescents of developed countries is an epidemic skin disease and has currently been linked to the Western diet (WD). It is the intention of this viewpoint to discuss the possible impact of WD-mediated nutrient signalling in the pathogenesis of acne. High glycaemic load and dairy protein consumption both increase insulin/insulin-like growth factor-1 (IGF-1) signalling (IIS) that is superimposed on elevated IGF-1 signalling of puberty. The cell's nutritional status is primarily sensed by the forkhead box transcription factor O1 (FoxO1) and the serine/threonine kinase mammalian target of rapamycin complex 1 (mTORC1). Increased IIS extrudes FoxO1 into the cytoplasm, whereas nuclear FoxO1 suppresses hepatic IGF-1 synthesis and thus impairs somatic growth. FoxO1 attenuates androgen signalling, interacts with regulatory proteins important for sebaceous lipogenesis, regulates the activity of innate and adaptive immunity, antagonizes oxidative stress and most importantly functions as a rheostat of mTORC1, the master regulator of cell growth, proliferation and metabolic homoeostasis. Thus, FoxO1 links nutrient availability to mTORC1-driven processes: increased protein and lipid synthesis, cell proliferation, cell differentiation including hyperproliferation of acroinfundibular keratinocytes, sebaceous gland hyperplasia, increased sebaceous lipogenesis, insulin resistance and increased body mass index. Enhanced androgen, TNF- and IGF-1 signalling due to genetic polymorphisms promoting the risk of acne all converge in mTORC1 activation, which is further enhanced by nutrient signalling of WD. Deeper insights into the molecular interplay of FoxO1/mTORC1-mediated nutrient signalling are thus of critical importance to understand the impact of WD on the promotion of epidemic acne and more serious mTORC1-driven diseases of civilization.
2013 John Wiley & Sons A/S.
Dietary intervention in acne: Attenuation of increased mTORC1 signaling promoted by Western diet.
The purpose of this paper is to highlight the endocrine signaling of Western diet, a fundamental environmental factor involved in the pathogenesis of epidemic acne. Western nutrition is characterized by high calorie uptake, high glycemic load, high fat and meat intake, as well as increased consumption of insulin- and IGF-1-level elevating dairy proteins. Metabolic signals of Western diet are sensed by the nutrient-sensitive kinase, mammalian target of rapamycin complex 1 (mTORC1), which integrates signals of cellular energy, growth factors (insulin, IGF-1) and protein-derived signals, predominantly leucine, provided in high amounts by milk proteins and meat. mTORC1 activates SREBP, the master transcription factor of lipogenesis. Leucine stimulates mTORC1-SREBP signaling and leucine is directly converted by sebocytes into fatty acids and sterols for sebaceous lipid synthesis. Over-activated mTORC1 increases androgen hormone secretion and most likely amplifies androgen-driven mTORC1 signaling of sebaceous follicles. Testosterone directly activates mTORC1. Future research should investigate the effects of isotretinoin on sebocyte mTORC1 activity. It is conceivable that isotretinoin may downregulate mTORC1 in sebocytes by upregulation of nuclear levels of FoxO1. The role of Western diet in acne can only be fully appreciated when all stimulatory inputs for maximal mTORC1 activation, i.e., glucose, insulin, IGF-1 and leucine, are adequately considered. Epidemic acne has to be recognized as an mTORC1-driven disease of civilization like obesity, type 2 diabetes, cancer and neurodegenerative diseases. These new insights into Western diet-mediated mTORC1-hyperactivity provide a rational basis for dietary intervention in acne by attenuating mTORC1 signaling by reducing (1) total energy intake, (2) hyperglycemic carbohydrates, (3) insulinotropic dairy proteins and (4) leucine-rich meat and dairy proteins. The necessary dietary changes are opposed to the evolution of industrialized food and fast food distribution of Westernized countries. An attenuation of mTORC1 signaling is only possible by increasing the consumption of vegetables and fruit, the major components of vegan or Paleolithic diets. The dermatologist bears a tremendous responsibility for his young acne patients who should be advised to modify their dietary habits in order to reduce activating stimuli of mTORC1, not only to improve acne but to prevent the harmful and expensive march to other mTORC1-related chronic diseases later in life.
FoxO, IGF-1, Western diet, acne, androgen, insulin, leucine, mTORC1, nutrition, prevention
Turning acne on/off via mTORC1.
Over the past 10 years, the increase in comprehension of the mechanisms behind acne has been truly exponential. Starting with the ethnological work of Cordain, accelerated by the epidemiological work of Adebamowo, supported by the clinical trials of Smith and Mann, Kwon, DiLandro and others, the interface of diet and acne is coming into focus. Melnik now presents an exceptional pair of papers that illustrate for dermatologists what translational research is all about. The Western diet, the role of dairy, FoxO1 and mTORC1, the interplay of agonists and antagonists, therapeutics present and future - the jigsaw puzzle is coming together.
2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd.
Full article: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3746129/
From the last article which is about the prior papers:
No doubt we have still more to learn, but this is a giant step forward. There have been 18, and likely will be more, conservative voices who insist on proof beyond doubt. Theirs will be a long wait. The design and conduct of a satisfactory prospective randomized clinical trial faces several unique challenges. It will require the recruitment of acne-prone individuals who do not yet have acne. They will need parents willing to have their children blindly consume real dairy products or counterfeits that have been tested as safe and healthy despite having been modified to remove all steroid hormones, growth hormones and other potential acnegens 19, without disturbing the taste and texture of the original. This is a tall order indeed, especially in the young and challenging population affected. Add into the equation the vast number of parents for whom dairy is beyond reproach as a perfect food. Top off the problem with a generation or two (or three) of physicians who believe the same, and one wonders if such a proposed study would ever pass through an institutional review board.
It is time to heed the words of Albert Kligman and strive to actually achieve the ultimate goal in medical practice, namely prevention 20."
At least that's supposed to be the goal. You just can't count on our doctors to help you achieve it. You have to do it yourself.
Also, See Istoretinoin (accutane) also works by impacting Fox01. But you can do it with diet. And intermittent fasting.
http://www.ncbi.nlm.nih.gov/pubmed/20930691
The role of transcription factor FoxO1 in the pathogenesis of acne vulgaris and the mode of isotretinoin action.
- Department of Dermatology, Environmental Medicine and Health Theory, University of Osnabruck, Germany. [email protected]
It is the purpose of this review to demonstrate that oral isotretinoin treatment restores all major pathogenetic factors of acne vulgaris by upregulation of the nuclear transcription factor FoxO1, which will be shown to be the major target of retinoid action. Nuclear FoxO1 deficiency is the result of increased growth factor signaling with activated phosphoinositol-3-kinase (PI3K) and Akt kinase during growth hormone signaling of puberty and increased insulin/IGF-1 signaling due to consumption of insulinotropic milk/dairy products as well as hyperglycemic carbohydrates of Western diet. Nuclear FoxO1 deficiency increases androgen receptor transactivation and modifies the activity of important nuclear receptors and key genes involved in pilosebaceous keratinocyte proliferation, sebaceous lipogenesis and expression of perifollicular inflammatory cytokines. Isotretinoin-induced upregulation of nuclear FoxO1 is proposed to be responsible for the mode of action of isotretinoin on all major pathogenetic factors in acne. Acne pathogenesis can be explained at the genomic level of transcriptional regulation. All major events in acne pathogenesis as well as all major effects of isotretinoin treatment appear to be related to modifications of the PI3K/Akt/FoxO1 signaling pathway, the well-known oncogenic pathway. These insights extend our understanding of FoxO1-mediated retinoid action in acne and other hyperproliferative skin diseases, cancer chemoprevention and cutaneous immune regulation. Understanding FoxOs pivotal regulatory role in acne allows the development of novel treatment strategies and dietary interventions in acne which focus on the restoration of growth factor- and diet-induced imbalances of nuclear FoxO protein levels.
PMID:20930691[PubMed - indexed for MEDLINE]
From the last article which is about the prior papers:
No doubt we have still more to learn, but this is a giant step forward. There have been 18, and likely will be more, conservative voices who insist on proof beyond doubt. Theirs will be a long wait. The design and conduct of a satisfactory prospective randomized clinical trial faces several unique challenges. It will require the recruitment of acne-prone individuals who do not yet have acne. They will need parents willing to have their children blindly consume real dairy products or counterfeits that have been tested as safe and healthy despite having been modified to remove all steroid hormones, growth hormones and other potential acnegens 19, without disturbing the taste and texture of the original. This is a tall order indeed, especially in the young and challenging population affected. Add into the equation the vast number of parents for whom dairy is beyond reproach as a perfect food. Top off the problem with a generation or two (or three) of physicians who believe the same, and one wonders if such a proposed study would ever pass through an institutional review board.
It is time to heed the words of Albert Kligman and strive to actually achieve the ultimate goal in medical practice, namely prevention 20."
One conceivable way to blind is to analyze the nutrition, enzymes, and hormones within milk and put it in water, then have a water placebo. It wouldn't be actual milk, and of course there would be a few limitations. However, it would be close and it would give us a general idea.
Another way would be to give the milk substitute and placebo to an older but acne-prone population. Giving certain foods/protocols to children has a higher chance of violating ethical guidelines than to those 18-21 years or older.
It would definitely be violating ethical guidelines if it required starving participants, no matter the age.
One thing's for certain before conducting such a study: participants must not be vitamin/mineral deficient. All of them must have had measured vitamin/mineral, hormone levels, and acne type/count before participating. All the parameters must be measured afterward, too. Ideally, the participants must have a controlled diet, or at least the authors should adjust for those confounding factors.
At least that's supposed to be the goal. You just can't count on our doctors to help you achieve it. You have to do it yourself.
There are some contraindications before going on such a diet. For example, those on chemotherapy (specifically, Bortezomib) can't drink green tea. Though drugs.com does provide a few food-drug interactions, it's not always reliable or accurate.
I actually own a copy of this commentary: http://www.ncbi.nlm.nih.gov/pubmed/20819084
Leyden JJ et al. raises a few good points. Namely, this one: "Demonstration of iso-tretinoin-induced elevation of FoxO1 levels in patients with acne is required before this intriguing possibility can be accepted...If a substantial body of evidence accumulates showing that FoxO1 levels are different in patients with acne compared with patients without acne, then the discussion can be elevated to that of a theory."
I'm not aware of any studies that actually measured FOX1 in patients.
At least that's supposed to be the goal. You just can't count on our doctors to help you achieve it. You have to do it yourself.
There are some contraindications before going on such a diet. For example, those on chemotherapy (specifically, Bortezomib) can't drink green tea. Though drugs.com does provide a few food-drug interactions, it's not always reliable or accurate.
.
What are you talking about?
At least that's supposed to be the goal. You just can't count on our doctors to help you achieve it. You have to do it yourself.
There are some contraindications before going on such a diet. For example, those on chemotherapy (specifically, Bortezomib) can't drink green tea. Though drugs.com does provide a few food-drug interactions, it's not always reliable or accurate.
.
What are you talking about?
I'm just saying that one should be careful and check for contraindications before going on any diet/lifestyle change. As you've indicated in your threads, there are some good foods, but not all those foods are compatible with certain diseases and/or medications.
Great summary of the recent research! Super helpful. I wrote a paper about acne & nutrition and came across the mTORC1 pathway and was fascinated. I think I'm going to focus on mTORC1 for my thesis paper but broaden the topic to include other diseases of civilization as well. Although I think there's enough to fill a whole book discussing mTORC1 and acne alone! It had to be 5-6 pages and there were specific things we HAD to talk about so I only mention mTORC1 briefly and I talk about supplement recommendations at the end because we had to ... I wanted to really focus on mTORC1! Glad to see other people fascinated in it as well.
Great summary of the recent research! Super helpful. I wrote a paper about acne & nutrition and came across the mTORC1 pathway and was fascinated. I think I'm going to focus on mTORC1 for my thesis paper but broaden the topic to include other diseases of civilization as well. Although I think there's enough to fill a whole book discussing mTORC1 and acne alone! Here's my paper on it. It had to be 5-6 pages and there were specific things we HAD to talk about so I only mention mTORC1 briefly and I talk about supplement recommendations at the end because we had to ... I wanted to really focus on mTORC1! Glad to see other people fascinated in it as well.
Nice paper. But in the paragraph starting with "Acne vulgaris, the most common form of acne affecting upwards of 85% of adolescents in Western countries (Melnik, 2012), has four fundamental physiological components". I.e. It's all about oily skin and bacteria that must be killed. I would say something to indicate that is the current accepted thinking. Since you later provide alternative causes, Such as the evidence that inflammatory events initiate acne formation. And the fact that you can have dry skin and acne.
Exp Dermatol. 2013 May;22(5):311-5. doi: 10.1111/exd.12142.Potential role of FoxO1 and mTORC1 in the pathogenesis of Western diet-induced acne.
AbstractAcne in adolescents of developed countries is an epidemic skin disease and has currently been linked to the Western diet (WD). It is the intention of this viewpoint to discuss the possible impact of WD-mediated nutrient signalling in the pathogenesis of acne. High glycaemic load and dairy protein consumption both increase insulin/insulin-like growth factor-1 (IGF-1) signalling (IIS) that is superimposed on elevated IGF-1 signalling of puberty. The cell's nutritional status is primarily sensed by the forkhead box transcription factor O1 (FoxO1) and the serine/threonine kinase mammalian target of rapamycin complex 1 (mTORC1). Increased IIS extrudes FoxO1 into the cytoplasm, whereas nuclear FoxO1 suppresses hepatic IGF-1 synthesis and thus impairs somatic growth. FoxO1 attenuates androgen signalling, interacts with regulatory proteins important for sebaceous lipogenesis, regulates the activity of innate and adaptive immunity, antagonizes oxidative stress and most importantly functions as a rheostat of mTORC1, the master regulator of cell growth, proliferation and metabolic homoeostasis. Thus, FoxO1 links nutrient availability to mTORC1-driven processes: increased protein and lipid synthesis, cell proliferation, cell differentiation including hyperproliferation of acroinfundibular keratinocytes, sebaceous gland hyperplasia, increased sebaceous lipogenesis, insulin resistance and increased body mass index. Enhanced androgen, TNF- and IGF-1 signalling due to genetic polymorphisms promoting the risk of acne all converge in mTORC1 activation, which is further enhanced by nutrient signalling of WD. Deeper insights into the molecular interplay of FoxO1/mTORC1-mediated nutrient signalling are thus of critical importance to understand the impact of WD on the promotion of epidemic acne and more serious mTORC1-driven diseases of civilization.
2013 John Wiley & Sons A/S.
Dermatoendocrinol. 2012 Jan 1;4(1):20-32. doi: 10.4161/derm.19828.Dietary intervention in acne: Attenuation of increased mTORC1 signaling promoted by Western diet.
AbstractThe purpose of this paper is to highlight the endocrine signaling of Western diet, a fundamental environmental factor involved in the pathogenesis of epidemic acne. Western nutrition is characterized by high calorie uptake, high glycemic load, high fat and meat intake, as well as increased consumption of insulin- and IGF-1-level elevating dairy proteins. Metabolic signals of Western diet are sensed by the nutrient-sensitive kinase, mammalian target of rapamycin complex 1 (mTORC1), which integrates signals of cellular energy, growth factors (insulin, IGF-1) and protein-derived signals, predominantly leucine, provided in high amounts by milk proteins and meat. mTORC1 activates SREBP, the master transcription factor of lipogenesis. Leucine stimulates mTORC1-SREBP signaling and leucine is directly converted by sebocytes into fatty acids and sterols for sebaceous lipid synthesis. Over-activated mTORC1 increases androgen hormone secretion and most likely amplifies androgen-driven mTORC1 signaling of sebaceous follicles. Testosterone directly activates mTORC1. Future research should investigate the effects of isotretinoin on sebocyte mTORC1 activity. It is conceivable that isotretinoin may downregulate mTORC1 in sebocytes by upregulation of nuclear levels of FoxO1. The role of Western diet in acne can only be fully appreciated when all stimulatory inputs for maximal mTORC1 activation, i.e., glucose, insulin, IGF-1 and leucine, are adequately considered. Epidemic acne has to be recognized as an mTORC1-driven disease of civilization like obesity, type 2 diabetes, cancer and neurodegenerative diseases. These new insights into Western diet-mediated mTORC1-hyperactivity provide a rational basis for dietary intervention in acne by attenuating mTORC1 signaling by reducing (1) total energy intake, (2) hyperglycemic carbohydrates, (3) insulinotropic dairy proteins and (4) leucine-rich meat and dairy proteins. The necessary dietary changes are opposed to the evolution of industrialized food and fast food distribution of Westernized countries. An attenuation of mTORC1 signaling is only possible by increasing the consumption of vegetables and fruit, the major components of vegan or Paleolithic diets. The dermatologist bears a tremendous responsibility for his young acne patients who should be advised to modify their dietary habits in order to reduce activating stimuli of mTORC1, not only to improve acne but to prevent the harmful and expensive march to other mTORC1-related chronic diseases later in life.
KEYWORDS:FoxO, IGF-1, Western diet, acne, androgen, insulin, leucine, mTORC1, nutrition, prevention
Exp Dermatol. 2013 Jul;22(7):505-6. doi: 10.1111/exd.12180.Turning acne on/off via mTORC1.
AbstractOver the past 10 years, the increase in comprehension of the mechanisms behind acne has been truly exponential. Starting with the ethnological work of Cordain, accelerated by the epidemiological work of Adebamowo, supported by the clinical trials of Smith and Mann, Kwon, DiLandro and others, the interface of diet and acne is coming into focus. Melnik now presents an exceptional pair of papers that illustrate for dermatologists what translational research is all about. The Western diet, the role of dairy, FoxO1 and mTORC1, the interplay of agonists and antagonists, therapeutics present and future - the jigsaw puzzle is coming together.
2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd.
Full article: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3746129/
Acne isn't just in the west. It's in every single country in the world - even in remote tanzanian tribes in africa acne is present (look up pictures if you refuse to believe me). It's ubiquitous, and has existed since the dawn of man. It's not just in "Murica" it's the world. Everybody on the planet experience zits from time to time it's only human. We are not meant to be perfect, we are designed to have flaws. if you're so obsessed with having entirely flawless skin than I suggest you move to south korea and hang with the skin care obsessed ,plastic surgery addicted, orthorexic women over in that country.
^Bubbles
You find pictures pictures of people with acne in remote tribes in their traditional diets in Tanzanian and share them. Go on. Let's see them.
No one in this thread is obsessed about anything except you with your obsessive trolling, attacks and insults. Acne is most prevalent by far in areas where they eat the current western diet or SAD and is rare to non-exist elsewhere and in the past.
Exp Dermatol. 2013 May;22(5):311-5. doi: 10.1111/exd.12142.Potential role of FoxO1 and mTORC1 in the pathogenesis of Western diet-induced acne.
AbstractAcne in adolescents of developed countries is an epidemic skin disease and has currently been linked to the Western diet (WD). It is the intention of this viewpoint to discuss the possible impact of WD-mediated nutrient signalling in the pathogenesis of acne. High glycaemic load and dairy protein consumption both increase insulin/insulin-like growth factor-1 (IGF-1) signalling (IIS) that is superimposed on elevated IGF-1 signalling of puberty. The cell's nutritional status is primarily sensed by the forkhead box transcription factor O1 (FoxO1) and the serine/threonine kinase mammalian target of rapamycin complex 1 (mTORC1). Increased IIS extrudes FoxO1 into the cytoplasm, whereas nuclear FoxO1 suppresses hepatic IGF-1 synthesis and thus impairs somatic growth. FoxO1 attenuates androgen signalling, interacts with regulatory proteins important for sebaceous lipogenesis, regulates the activity of innate and adaptive immunity, antagonizes oxidative stress and most importantly functions as a rheostat of mTORC1, the master regulator of cell growth, proliferation and metabolic homoeostasis. Thus, FoxO1 links nutrient availability to mTORC1-driven processes: increased protein and lipid synthesis, cell proliferation, cell differentiation including hyperproliferation of acroinfundibular keratinocytes, sebaceous gland hyperplasia, increased sebaceous lipogenesis, insulin resistance and increased body mass index. Enhanced androgen, TNF- and IGF-1 signalling due to genetic polymorphisms promoting the risk of acne all converge in mTORC1 activation, which is further enhanced by nutrient signalling of WD. Deeper insights into the molecular interplay of FoxO1/mTORC1-mediated nutrient signalling are thus of critical importance to understand the impact of WD on the promotion of epidemic acne and more serious mTORC1-driven diseases of civilization.
2013 John Wiley & Sons A/S.
Dermatoendocrinol. 2012 Jan 1;4(1):20-32. doi: 10.4161/derm.19828.Dietary intervention in acne: Attenuation of increased mTORC1 signaling promoted by Western diet.
AbstractThe purpose of this paper is to highlight the endocrine signaling of Western diet, a fundamental environmental factor involved in the pathogenesis of epidemic acne. Western nutrition is characterized by high calorie uptake, high glycemic load, high fat and meat intake, as well as increased consumption of insulin- and IGF-1-level elevating dairy proteins. Metabolic signals of Western diet are sensed by the nutrient-sensitive kinase, mammalian target of rapamycin complex 1 (mTORC1), which integrates signals of cellular energy, growth factors (insulin, IGF-1) and protein-derived signals, predominantly leucine, provided in high amounts by milk proteins and meat. mTORC1 activates SREBP, the master transcription factor of lipogenesis. Leucine stimulates mTORC1-SREBP signaling and leucine is directly converted by sebocytes into fatty acids and sterols for sebaceous lipid synthesis. Over-activated mTORC1 increases androgen hormone secretion and most likely amplifies androgen-driven mTORC1 signaling of sebaceous follicles. Testosterone directly activates mTORC1. Future research should investigate the effects of isotretinoin on sebocyte mTORC1 activity. It is conceivable that isotretinoin may downregulate mTORC1 in sebocytes by upregulation of nuclear levels of FoxO1. The role of Western diet in acne can only be fully appreciated when all stimulatory inputs for maximal mTORC1 activation, i.e., glucose, insulin, IGF-1 and leucine, are adequately considered. Epidemic acne has to be recognized as an mTORC1-driven disease of civilization like obesity, type 2 diabetes, cancer and neurodegenerative diseases. These new insights into Western diet-mediated mTORC1-hyperactivity provide a rational basis for dietary intervention in acne by attenuating mTORC1 signaling by reducing (1) total energy intake, (2) hyperglycemic carbohydrates, (3) insulinotropic dairy proteins and (4) leucine-rich meat and dairy proteins. The necessary dietary changes are opposed to the evolution of industrialized food and fast food distribution of Westernized countries. An attenuation of mTORC1 signaling is only possible by increasing the consumption of vegetables and fruit, the major components of vegan or Paleolithic diets. The dermatologist bears a tremendous responsibility for his young acne patients who should be advised to modify their dietary habits in order to reduce activating stimuli of mTORC1, not only to improve acne but to prevent the harmful and expensive march to other mTORC1-related chronic diseases later in life.
KEYWORDS:FoxO, IGF-1, Western diet, acne, androgen, insulin, leucine, mTORC1, nutrition, prevention
Exp Dermatol. 2013 Jul;22(7):505-6. doi: 10.1111/exd.12180.Turning acne on/off via mTORC1.
AbstractOver the past 10 years, the increase in comprehension of the mechanisms behind acne has been truly exponential. Starting with the ethnological work of Cordain, accelerated by the epidemiological work of Adebamowo, supported by the clinical trials of Smith and Mann, Kwon, DiLandro and others, the interface of diet and acne is coming into focus. Melnik now presents an exceptional pair of papers that illustrate for dermatologists what translational research is all about. The Western diet, the role of dairy, FoxO1 and mTORC1, the interplay of agonists and antagonists, therapeutics present and future - the jigsaw puzzle is coming together.
2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd.
Full article: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3746129/
Acne isn't just in the west. It's in every single country in the world - even in remote tanzanian tribes in africa acne is present (look up pictures if you refuse to believe me). It's ubiquitous, and has existed since the dawn of man. It's not just in "Murica" it's the world. Everybody on the planet experience zits from time to time it's only human. We are not meant to be perfect, we are designed to have flaws. if you're so obsessed with having entirely flawless skin than I suggest you move to south korea and hang with the skin care obsessed ,plastic surgery addicted, orthorexic women over in that country.
You are completely wrong.
http://archderm.jamanetwork.com/article.aspx?articleid=479093
Here is a summary of the paper -
Background In westernized societies, acne vulgaris is a nearly universal skin disease afflicting 79% to 95% of the adolescent population. In men and women older than 25 years, 40% to 54% have some degree of facial acne, and clinical facial acne persists into middle age in 12% of women and 3% of men. Epidemiological evidence suggests that acne incidence rates are considerably lower in nonwesternized societies. Herein we report the prevalence of acne in 2 nonwesternized populations: the Kitavan Islanders of Papua New Guinea and the Ache hunter-gatherers of Paraguay. Additionally, we analyze how elements in nonwesternized environments may influence the development of acne.
Observations Of 1200 Kitavan subjects examined (including 300 aged 15-25 years), no case of acne (grade 1 with multiple comedones or grades 2-4) was observed. Of 115 Ache subjects examined (including 15 aged 15-25 years) over 843 days, no case of active acne (grades 1-4) was observed.
Conclusions The astonishing difference in acne incidence rates between nonwesternized and fully modernized societies cannot be solely attributed to genetic differences among populations but likely results from differing environmental factors. Identification of these factors may be useful in the treatment of acne in Western populations.
From an article about preventing cancer, especially breast cancer as a better thing to do than expose your self to radiation in annual screenings prone to both false positives and failures to catch cancers at their early stages.
Limit your protein. Newer research has emphasized the importance of the mTOR pathways. When these are active, cancer growth is accelerated. One way to quiet this pathway is by limiting your protein, so that your body has enough protein for cellular turnover and muscle maintenance, but not more. Experts like Dr. Ron Rosedale believe an ideal amount for many would be around one gram of protein per kilogram of lean body mass, or roughly a bit less than half a gram of protein per every pound of lean body weight. For most people, this ranges between 40 and 70 grams of protein a day, which is typically about two-thirds to half of what they are currently consuming.